Recognizing Pre-Eclampsia Symptoms with Diabetes
Learn pre-eclampsia symptoms during pregnancy with diabetes, the red flags that need immediate care, and why gestational, T1D, and T2D raise the risk.

In this article(29)
A blood pressure reading higher than usual. A headache that will not quit. Swelling in your face that looks different from the swelling in your ankles. During pregnancy, any one of these can be normal, but pre-eclampsia symptoms often start exactly this way, and recognizing them early matters even more when you have diabetes. Pre-eclampsia is a pregnancy complication marked by high blood pressure and signs of organ stress, usually after 20 weeks, and diabetes meaningfully raises the risk. Most cases are caught early at routine prenatal visits, and quick action protects both you and your baby.
This guide walks through what to watch for, the red flags that mean call your provider now, and why gestational, type 1, and type 2 diabetes each push the risk higher. We will keep it practical, since the most useful thing during a busy pregnancy is knowing exactly when to pick up the phone.
What Are the Signs of Pre-Eclampsia
The first thing to know about pre-eclampsia symptoms is that they often build quietly, which is why prenatal blood pressure checks are not optional. The American College of Obstetricians and Gynecologists lists the following as the core diagnostic features after 20 weeks of pregnancy:
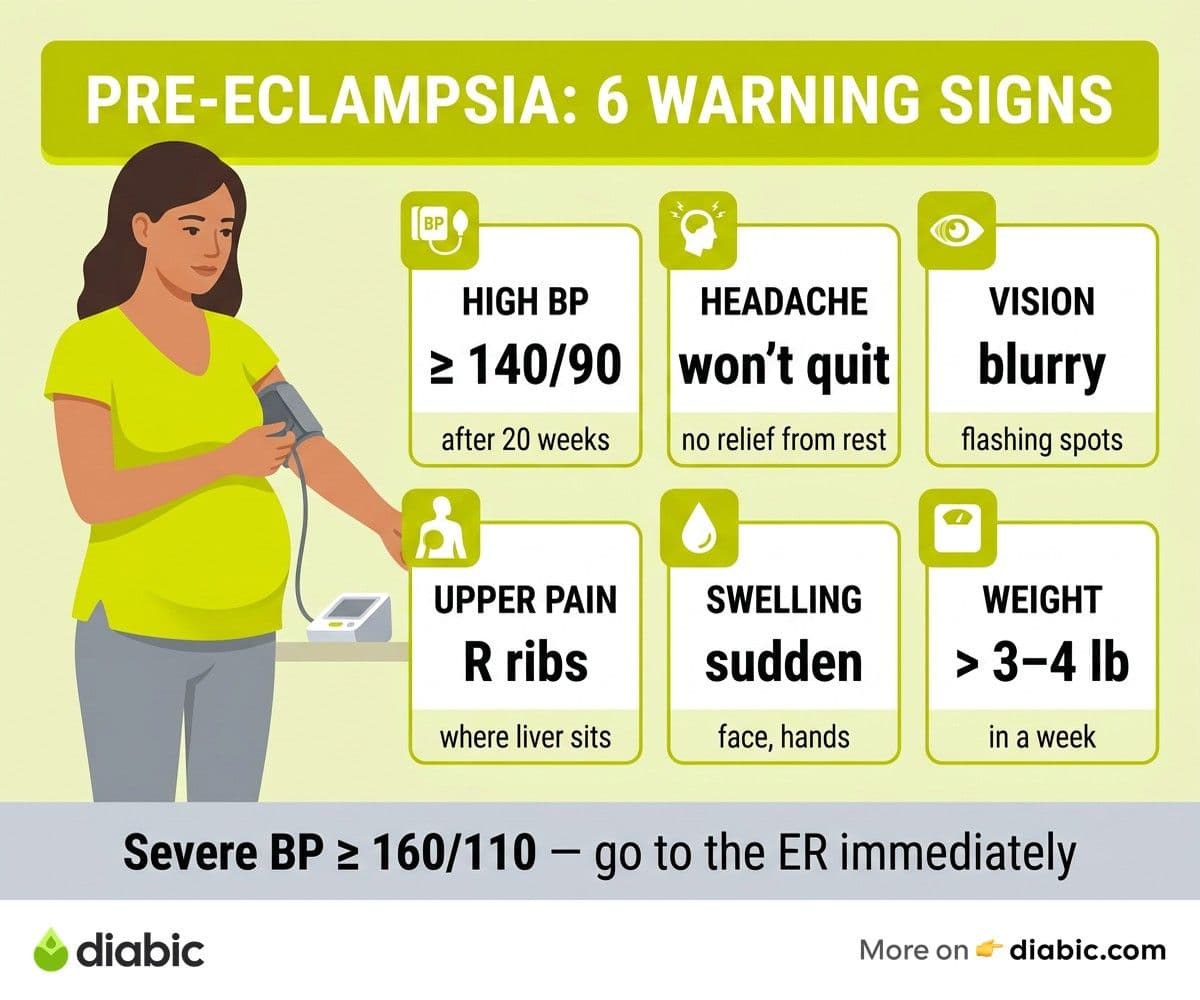
- High blood pressure of 140/90 mmHg or above on two readings taken at least four hours apart, or a single severe reading of 160/110 mmHg or higher
- Protein in the urine, detected through a routine dipstick test or 24-hour collection
- Severe headaches that do not improve with rest, fluids, or acetaminophen
- Vision changes, including blurred vision, seeing flashing spots, or temporary loss of vision
- Upper abdominal pain, especially under the right ribs, where the liver sits
- Swelling in the face and hands that develops suddenly or feels different from typical pregnancy swelling
Sudden weight gain of more than three to four pounds in a week, persistent nausea late in pregnancy, and shortness of breath are also worth flagging. None of these signs diagnose the condition on their own, but the combination, especially with elevated blood pressure, calls for prompt evaluation.
Pre-Eclampsia Symptoms and Signs to Watch For
The warning signs can develop on two different timelines, and knowing this helps you trust your instincts about what feels off.
How symptoms can develop gradually or suddenly
Some people experience a slow rise in blood pressure across several weeks, with mild symptoms appearing one at a time. Others move quickly from feeling fine to feeling unwell within days, sometimes hours. Both patterns are real, and neither means you missed something. The Preeclampsia Foundation emphasizes that any new or worsening symptom in the second half of pregnancy deserves a call to your provider, not a wait-and-see approach.
Why some signs overlap with normal pregnancy discomforts
Pregnancy itself causes ankle swelling, occasional headaches, fatigue, and reflux. So how do you tell what is concerning? A few patterns help:
- Swelling that suddenly extends to your face, eyelids, or hands and does not improve with rest
- Headaches that resist your usual remedies and last more than a few hours
- Vision changes, which are not part of typical pregnancy
- Pain in the upper right abdomen, which is not common from baby movement
When in doubt, call. This is not something providers want you to figure out at home.
The difference between mild and severe pre-eclampsia
ACOG describes pre-eclampsia with severe features as having any of the following: blood pressure of 160/110 or higher, severely impaired liver or kidney function, low platelet counts, fluid in the lungs, severe headache or vision changes, or upper abdominal pain. Severe pre-eclampsia usually requires hospital admission and may lead to earlier delivery to protect both you and your baby. The mild form involves the diagnostic criteria without these severe features and may be managed with closer monitoring, depending on how far along you are.
What Are the Signs of Pre-Eclampsia with Gestational Diabetes
Pre-eclampsia and gestational diabetes are connected through shared underlying mechanisms. Both involve changes in how blood vessels and the placenta respond to pregnancy hormones, and the two often appear together.
How gestational diabetes increases pre-eclampsia risk
Research summarized by the American Diabetes Association shows that gestational diabetes roughly doubles the risk of pre-eclampsia compared to pregnancies without it. Insulin resistance, elevated blood glucose, and changes in placental blood flow all contribute. Higher pre-pregnancy weight and pre-existing high blood pressure further raise the combined risk.
Symptoms that overlap between the two conditions
Both conditions can cause swelling, fatigue, and changes in how you feel after meals. The signs that point specifically to pre-eclampsia, rather than gestational diabetes, are:
- New or rising blood pressure readings, since gestational diabetes alone does not raise blood pressure
- Severe headaches and vision changes
- Upper abdominal pain
- Sudden facial or hand swelling
If you are managing gestational diabetes and notice any of these, contact your prenatal team. The fact that you already have one pregnancy condition makes these warning signs harder to dismiss, not easier.
Why closer monitoring is recommended when both are present
Most providers schedule more frequent visits, additional blood pressure checks, and earlier or repeated urine protein testing for people managing gestational diabetes. Some recommend home blood pressure monitoring as well, which we will cover below. Closer monitoring is not because something is wrong, it is because catching a problem early gives the best outcomes.
Does Diabetes Increase the Risk of Pre-Eclampsia
Yes, all forms of diabetes during pregnancy raise the risk, though the level of risk varies. Understanding why blood pressure and diabetes both matter helps explain the mechanism.
Research data on diabetes and pre-eclampsia risk
According to the Centers for Disease Control and Prevention and major obstetric studies, pregnancies complicated by pre-existing diabetes carry roughly a two to four times higher risk compared to pregnancies without diabetes. Gestational diabetes increases the risk by roughly 1.5 to 2 times. The combination of vascular changes, kidney involvement, and metabolic stress all contribute.
Type 1, type 2, and gestational diabetes risk levels
Each form carries a slightly different risk pattern:
- Type 1 diabetes: Risk is highest when there is pre-existing kidney involvement, a history of high blood pressure, or A1C above target heading into pregnancy. Tighter glucose management before and during pregnancy may help reduce risk.
- Type 2 diabetes: Risk also rises with age, weight, pre-existing hypertension, and longer diabetes duration. Many people with type 2 also have other cardiovascular risk factors, which compound the picture.
- Gestational diabetes: Risk is lower than with pre-existing diabetes but still meaningfully elevated. Diet, exercise, and glucose targets agreed with your team can reduce risk further.
The role of blood pressure management in reducing risk
Blood pressure is one of the most actionable levers. Your prenatal team may recommend how diabetes causes high blood pressure education, low-dose aspirin starting between weeks 12 and 16 if your risk is elevated, and adjustments to existing blood pressure medication if needed. Talk to your doctor before starting or changing any medication during pregnancy. Some blood pressure medications are safe in pregnancy and others are not.
From my experience: Living with type 1 diabetes for fourteen years has taught me to respect overlapping conditions. When my partner was pregnant and managing gestational diabetes, the most useful tool we had was a basic home blood pressure cuff and a simple log on the fridge. Twice a day, same arm, same chair. It was not high-tech, but it caught a slow upward drift two weeks before her routine visit and gave her care team time to act calmly rather than urgently. If you take one habit from this article, that is the one I would pick.
Blood Pressure Monitoring During Pregnancy
For anyone with diabetes who is pregnant or planning a pregnancy, blood pressure monitoring is one of the most important habits to build early. The relationship between blood pressure, diabetes, and pregnancy outcomes is direct: better readings, better outcomes.
How often blood pressure should be checked
Routine prenatal visits already include a blood pressure check. For people with diabetes or other risk factors, providers often recommend additional readings between visits, especially in the third trimester. If your readings have been consistently normal, weekly home checks may be enough. If they have been climbing, daily monitoring may be advised.
Home blood pressure monitoring during pregnancy
A few practical tips for home monitoring:
- Use a validated upper-arm cuff, not a wrist cuff, since wrist devices are less reliable
- Sit quietly for five minutes before measuring, with feet flat and back supported
- Take two readings a minute apart and record both, along with the time and arm used
- Bring your log to every prenatal visit so your provider can see the trend, not just snapshots
The National Heart, Lung, and Blood Institute provides plain-language guides on technique that are worth reading once before you start.
When blood pressure changes signal a concern
Call your provider if you see:
- Two consecutive readings of 140/90 mmHg or higher
- A single reading of 160/110 mmHg or higher
- Readings that climb steadily across several days, even if individual numbers are below 140/90
- Any high reading combined with a symptom from the earlier list (headache, vision changes, upper abdominal pain, swelling)
Do not wait for your next scheduled visit if any of these occur. Evaluation is straightforward and quick, and your team would rather rule it out than miss it.
What to Do If You Suspect Pre-Eclampsia
If you think you might be experiencing this condition, the action plan is simple, and acting quickly is the most important thing you can do.
When to contact your provider immediately
Call right away or go to the labor and delivery unit if you have any of the following after 20 weeks of pregnancy:
- A severe headache that does not respond to rest or acetaminophen
- Vision changes (blurred vision, flashing spots, partial vision loss)
- Severe upper abdominal or right-sided pain
- Sudden severe swelling of face or hands
- Shortness of breath that is new or worsening
- Blood pressure of 160/110 mmHg or higher on a home reading
- Decreased fetal movement compared to your usual pattern
If you cannot reach your provider quickly, go to the labor and delivery triage unit at your delivery hospital. They are open around the clock and trained to evaluate exactly this.
What happens at the hospital evaluation process
Evaluation typically includes:
- Repeat blood pressure measurements, often over a couple of hours
- Urine testing for protein, sometimes with a 24-hour collection
- Blood tests to check liver function, kidney function, and platelets
- Fetal monitoring to assess the baby's heart rate and movement
- An ultrasound if there are concerns about growth or amniotic fluid
If the diagnosis is confirmed, the team will discuss next steps based on how severe it is, how far along you are, and how stable both you and the baby look.
Treatment options and delivery planning
Treatment depends on severity and gestational age. Options can include closer monitoring, medication to lower blood pressure, magnesium sulfate to prevent seizures in severe cases, and delivery, which is the only definitive cure. According to the National Institute of Diabetes and Digestive and Kidney Diseases, people with diabetes need additional attention during this period, since blood sugar can shift quickly when other conditions are being treated.
If you have pre-existing kidney involvement, our guide on managing kidney health with diabetes covers how kidney function fits into the larger picture and what your team is monitoring.
Why early detection dramatically improves outcomes
Caught early, this condition is highly manageable. Most pregnancies complicated by it result in healthy babies and full recovery for the parent, especially when symptoms are flagged before they progress. The window between mild and severe disease is the window where calm management is possible. That window is what your prenatal visits and home monitoring exist to protect.
Frequently Asked Questions
What are the signs of pre-eclampsia with gestational diabetes?
Signs include sudden high blood pressure, protein in the urine, severe headaches, vision changes, and upper abdominal pain. Having gestational diabetes increases the risk, making regular blood pressure monitoring especially important throughout the second half of pregnancy.
Does diabetes increase the risk of pre-eclampsia?
Yes. All forms of diabetes during pregnancy, including gestational, type 1, and type 2, increase the risk. Good blood sugar and blood pressure management may help reduce this risk, and your prenatal team can tailor a monitoring plan that fits your situation.
Can pre-eclampsia happen after delivery?
Yes. Postpartum pre-eclampsia can develop within 48 hours after delivery and occasionally up to six weeks later. Symptoms are similar to those during pregnancy. If you experience severe headache, vision changes, or new swelling after delivery, contact your provider promptly.
How is pre-eclampsia treated when you have diabetes?
Treatment includes managing blood pressure, monitoring blood sugar more closely, and in many cases planning delivery once the baby is mature enough. The combination requires coordination between your obstetric and diabetes teams. Talk to your doctor about how each medication and monitoring decision fits into your existing diabetes plan.
Will I have pre-eclampsia again in a future pregnancy?
Having pre-eclampsia in one pregnancy raises the risk in future pregnancies, especially when diabetes is also present. Pre-pregnancy planning, blood pressure management, and discussion of low-dose aspirin with your provider can all reduce that risk.
Where to Go from Here
If you are pregnant with diabetes, the most important habit you can build this week is consistent blood pressure monitoring and a clear list of warning signs that should prompt a call. Print the red-flag list, stick it on the fridge, and share it with your partner or a trusted family member so you have backup if symptoms appear. Pre-eclampsia symptoms are far more manageable when caught early, and the partnership between you, your prenatal team, and your diabetes team is what makes early detection possible.
For more on the connection between diabetes and cardiovascular health, our blood pressure cluster covers diet, medication, and natural strategies that fit different life stages, and our kidney health resources cover the related territory of long-term protection. Small, consistent habits add up, and they protect what matters most.
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetic Dental Checkup Frequency: How Often to Go
Diabetic dental checkup frequency matters more than most people realize. Learn how often to visit, what to expect, and how to protect your oral health.

Oral Thrush and Diabetes: Causes and Treatment
Oral thrush diabetes connection explained, plus symptoms, antifungal treatment options, and how to keep this fungal infection from coming back.

Diabetes and Gum Disease: Causes and Prevention
Diabetes gum disease runs both ways. Learn why diabetes raises the risk, how gum infection affects blood sugar, and prevention steps that may help.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.