Hashimoto's and Type 1 Diabetes: The Autoimmune Link
Hashimoto's and type 1 diabetes share genetic roots and often co-occur. Learn the autoimmune link, screening guidance, and how to manage both.

In this article(23)
Hashimoto's and type 1 diabetes share more than just the label "autoimmune." The two conditions co-occur at a surprisingly high rate, and once you understand why, the rest of the picture starts to make sense.
If you live with type 1 diabetes, your risk of developing Hashimoto's thyroiditis is much higher than the general population. Catching it early can mean fewer days of unexplained fatigue, more stable blood sugar, and a smoother experience at the endocrinologist's office. This guide walks through the science behind the connection, what screening looks like, and how to manage both conditions without losing your mind.
Why Do Hashimoto's and Type 1 Diabetes Often Coexist
Both conditions belong to the same family of disorders, where the immune system mistakenly attacks healthy tissue. In type 1 diabetes, the target is the insulin-producing beta cells in the pancreas. In Hashimoto's thyroiditis, the target is the thyroid gland. The shared mechanism explains why they so often travel together.
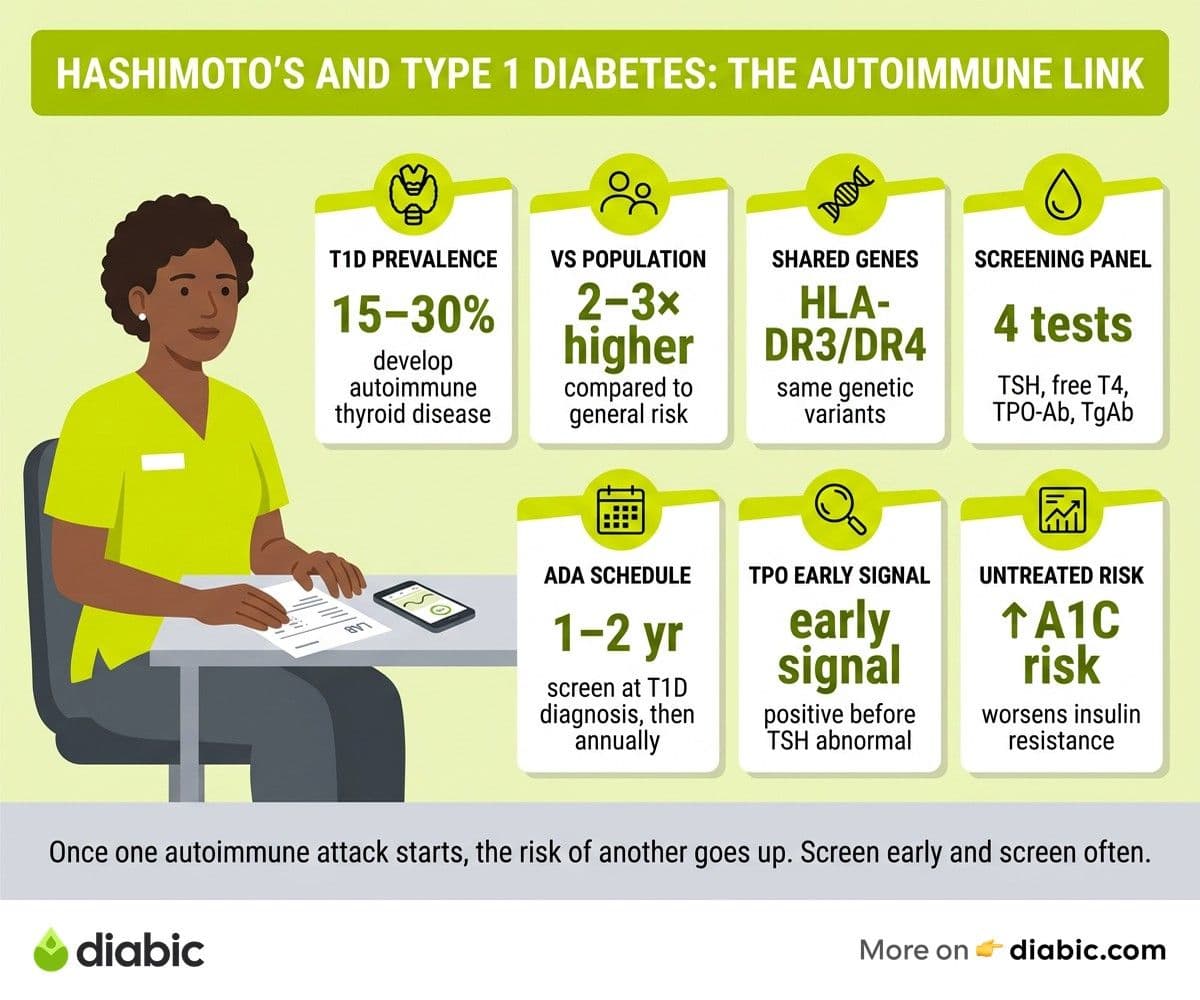
Genetics plays a large role. Specific variants of the human leukocyte antigen (HLA) genes, especially HLA-DR3 and HLA-DR4, raise the risk of multiple autoimmune conditions at once. According to a review in Endocrine Reviews, people with one autoimmune endocrine disease are several times more likely to develop another, a phenomenon known as autoimmune polyendocrine syndrome.
Prevalence numbers tell the story clearly. Studies cited by the American Thyroid Association and other endocrine bodies report that 15 to 30 percent of people with type 1 diabetes also develop autoimmune thyroid disease, with Hashimoto's being the most common form. That rate is roughly two to three times higher than what you would see in the general population.
The clustering is not random. Once one immune misfire happens, the same genetic and environmental triggers that started the first attack can set off another. Viral infections, gut microbiome changes, vitamin D deficiency, and chronic stress have all been studied as possible contributors.
Should Type 1 people with diabetes Be Screened for Hashimoto's
Yes, and the recommendation comes straight from the American Diabetes Association. The ADA Standards of Care advise screening for thyroid dysfunction at the time of type 1 diabetes diagnosis, and then periodically afterward, even when no symptoms are present.
The reason is simple. Hashimoto's often develops slowly, with symptoms that overlap heavily with everyday life: tiredness, weight changes, brain fog, feeling cold. People with diabetes already deal with fatigue and energy swings, so a creeping thyroid problem can hide for years before anyone connects the dots.
How Often Screening Should Happen
Most endocrinologists check thyroid function every one to two years for people with type 1 diabetes who have no symptoms. If antibodies are detected, or if you start showing symptoms, testing happens more frequently. New parents diagnosing a child with type 1 are usually offered thyroid screening at the first hospital visit, then annually.
What Tests Are Used
The standard panel includes:
- TSH (thyroid-stimulating hormone): the most sensitive marker of thyroid function. A high TSH suggests the thyroid is underactive.
- Free T4: measures the active thyroid hormone in your blood.
- Thyroid peroxidase antibodies (TPO-Ab): the autoimmune marker. Elevated TPO-Ab confirms an autoimmune cause like Hashimoto's.
- Thyroglobulin antibodies (TgAb): a secondary autoimmune marker.
If you want a deeper breakdown of what these numbers mean, our guide on what a TSH test means for diabetes walks through the ranges and how to interpret your results.
Why Early Detection Matters
Untreated Hashimoto's gradually slows your metabolism. That can cause weight gain, raise cholesterol, worsen insulin sensitivity, and quietly destabilize blood sugar. Catching it before symptoms get severe means treatment is simpler, dosing is more predictable, and your diabetes management stays on track.
Understanding the Autoimmune Connection
Autoimmunity happens when the immune system, which normally fights infections, starts attacking the body's own cells. Researchers still debate the exact triggers, but a combination of genetic susceptibility and environmental exposure seems to set the process in motion.
In type 1 diabetes, immune cells called T-lymphocytes infiltrate the pancreas and destroy beta cells. Without beta cells, the body cannot produce insulin, and external insulin becomes essential for survival. The NIDDK explains this process in detail and notes that the autoimmune attack often begins years before symptoms appear.
Hashimoto's follows a similar pattern. Lymphocytes infiltrate the thyroid gland, gradually destroying its ability to produce thyroid hormone. Over time, hormone output drops, and hypothyroidism develops. The Mayo Clinic describes Hashimoto's as the most common cause of hypothyroidism in countries with adequate iodine intake.
The reason these two conditions overlap is shared immunology. The same genetic variants that make beta cells vulnerable also make thyroid cells vulnerable. Once the immune system has crossed the line and started attacking self-tissue, it is more likely to do so again somewhere else.
From my experience: I was diagnosed with type 1 diabetes at 17, and seven years later my routine bloodwork came back with a high TSH and elevated TPO antibodies. I had been chalking up the constant cold hands and afternoon energy crashes to long workdays. Starting levothyroxine was not dramatic, but within a few months my fatigue lifted and my CGM graphs got noticeably less spiky. I now ask for thyroid labs every year without waiting for the doctor to suggest it.
Hashimoto's Thyroiditis and Diabetes Management
When Hashimoto's progresses to hypothyroidism, blood sugar management gets harder, even if your insulin doses and routine have not changed. The thyroid sets the pace for your metabolism, so when it slows down, glucose moves through the body differently.
People with hypothyroidism tend to absorb carbohydrates more slowly and clear glucose from the bloodstream less efficiently. The result is often a flatter blood sugar curve early after meals, followed by a longer, more drawn-out rise. For people on insulin, that can lead to lows in the first hour after eating and stubborn highs three to four hours later.
A study published in Diabetes Care found that people with both type 1 diabetes and untreated hypothyroidism had higher rates of hypoglycemia and more variable A1C readings compared to those with normal thyroid function. Treating the thyroid often improved their glucose stability within a few months.
Hashimoto's also affects how the liver handles glucose, the way muscles take up insulin, and how cortisol responds to stress. The cumulative effect is small for some people and significant for others, which is why individualized lab follow-up is so important.
Hypothyroidism and Diabetes: The Practical Impact
The everyday symptoms of hypothyroidism overlap heavily with both poor diabetes management and ordinary life stress, which is part of why it gets missed. Fatigue, brain fog, dry skin, hair thinning, weight gain, feeling cold all the time, constipation, and low mood are all common.
Many people assume their tiredness is from work, parenting, or running blood sugar a bit high. That guess is sometimes right, but if the symptoms persist after diabetes management improves, thyroid function is worth checking.
Weight Changes and Energy Levels
Hypothyroidism slows resting metabolism, so weight can creep up even when calorie intake has not changed. Combined with the natural weight effects of insulin therapy, the result can feel discouraging. The fix is usually thyroid hormone replacement, not stricter dieting.
Mood and Mental Clarity
Low thyroid hormone affects neurotransmitter balance, which can mimic or worsen depression and anxiety. Diabetes already increases the risk of mood disorders, and untreated hypothyroidism stacks the deck further. Mental health that improves after starting levothyroxine is a strong sign that thyroid function was a contributing factor.
How Treatment Affects Blood Sugar
Starting levothyroxine can change insulin requirements within a few weeks. Some people find their basal needs go up modestly as metabolism speeds back to normal. Others see more stable post-meal numbers without needing to change anything. Talk to your diabetes care team before, during, and after starting thyroid medication so dose adjustments happen safely.
For a deeper look at the day-to-day side of this, see our guide on how thyroid affects blood sugar.
Managing Both Conditions Together
Living with two autoimmune conditions does not have to mean living at the doctor's office. With a steady routine and clear communication, most people manage both well.
Coordinating Care
An endocrinologist can usually manage both diabetes and thyroid disease, which simplifies follow-up and lab ordering. If your diabetes care comes from a primary care provider, ask whether they are comfortable monitoring thyroid function as well or whether a referral makes sense.
Make sure both conditions show up on every visit's problem list, and that whoever orders your annual labs knows to include TSH and a thyroid antibody panel periodically.
Medication Timing
Levothyroxine is best absorbed on an empty stomach, typically 30 to 60 minutes before breakfast. Coffee, calcium, and iron supplements can blunt absorption, so they should be spaced apart from the morning dose. People who take metformin or other oral diabetes drugs do not usually need to adjust timing relative to thyroid medication, but it is worth confirming with your pharmacist.
Monitoring Both Conditions
Most people benefit from:
- A1C every three to six months to track diabetes management.
- TSH every six to twelve months once thyroid levels are stable.
- Thyroid antibodies if there is a flare in symptoms or new diagnosis is suspected.
- Lipid panel and vitamin D annually, since both conditions can affect these markers.
A continuous glucose monitor (CGM) can be especially helpful during thyroid dose changes, because it shows the day-to-day patterns that single fingersticks miss.
Building a Sustainable Routine
The combination of two chronic conditions is more sustainable when daily habits are predictable. Eating at consistent times, sleeping seven to nine hours, taking medications on schedule, and moving daily all help both conditions at once. Stress management matters too, because cortisol affects both blood sugar and the autoimmune process.
For more on coordinated care and day-to-day strategies, see our piece on managing hypothyroidism and diabetes together.
A Practical Next Step
If you live with type 1 diabetes and have not had thyroid labs in the past year, ask for them at your next visit. A simple TSH test can rule out the most common issues, and if antibodies are added, you get a clearer picture of any underlying autoimmune activity. Catching Hashimoto's early is one of the easier wins in diabetes care, and the peace of mind is worth the extra blood draw.
FAQ
Why do Hashimoto's and type 1 diabetes often coexist?
Both conditions are driven by autoimmune processes and share genetic risk factors, particularly certain HLA gene variants. Having one autoimmune condition significantly increases the likelihood of developing another, a pattern known as autoimmune polyendocrine syndrome.
Should type 1 people with diabetes be screened for Hashimoto's?
Yes. The ADA recommends thyroid function screening at type 1 diabetes diagnosis and periodically thereafter, typically every one to two years. Early detection of Hashimoto's allows for prompt treatment that improves both thyroid health and diabetes management.
What are the first signs of Hashimoto's in someone with type 1 diabetes?
Common early signs include unusual fatigue, sensitivity to cold, dry skin, weight gain, brain fog, and unexplained changes in insulin needs. Because these symptoms overlap with diabetes itself, lab testing is the only reliable way to confirm.
Does Hashimoto's affect insulin requirements?
It can. Untreated hypothyroidism often slows glucose metabolism and may increase the risk of hypoglycemia. Once levothyroxine restores thyroid levels, insulin needs may rise modestly and blood sugar typically becomes more stable.
Can children with type 1 diabetes get Hashimoto's?
Yes, and pediatric endocrinologists routinely screen for it. The combination is more common in girls and tends to appear during adolescence, which is why annual thyroid checks are part of standard pediatric type 1 care.
The honest summary on Hashimoto's and type 1 diabetes is that the two conditions overlap often enough to deserve standing screening rather than symptom-led testing. A yearly TSH and antibody panel takes one extra blood tube, and catching thyroid involvement early usually means smoother insulin dosing, steadier energy, and fewer mystery weeks where nothing seems to work.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetic Dental Checkup Frequency: How Often to Go
Diabetic dental checkup frequency matters more than most people realize. Learn how often to visit, what to expect, and how to protect your oral health.

Oral Thrush and Diabetes: Causes and Treatment
Oral thrush diabetes connection explained, plus symptoms, antifungal treatment options, and how to keep this fungal infection from coming back.

Diabetes and Gum Disease: Causes and Prevention
Diabetes gum disease runs both ways. Learn why diabetes raises the risk, how gum infection affects blood sugar, and prevention steps that may help.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.