Blood Pressure and Diabetes: Why Both Matter
Blood pressure diabetes risks compound when both go unchecked. Learn how the two conditions affect each other and why managing them together protects you.

In this article(10)
Managing blood pressure and diabetes together is not the same as managing each one separately. When the two conditions overlap, the risks to your heart, kidneys, and eyes do not just add up. They multiply. Understanding the blood pressure diabetes connection is one of the most useful things you can do for your long-term health, because the same actions that lower one usually help the other.
This post walks through why these two conditions are so often paired, how they damage your body in similar ways, and what a coordinated approach to managing them looks like in real life.
The Blood Pressure Diabetes Connection Explained
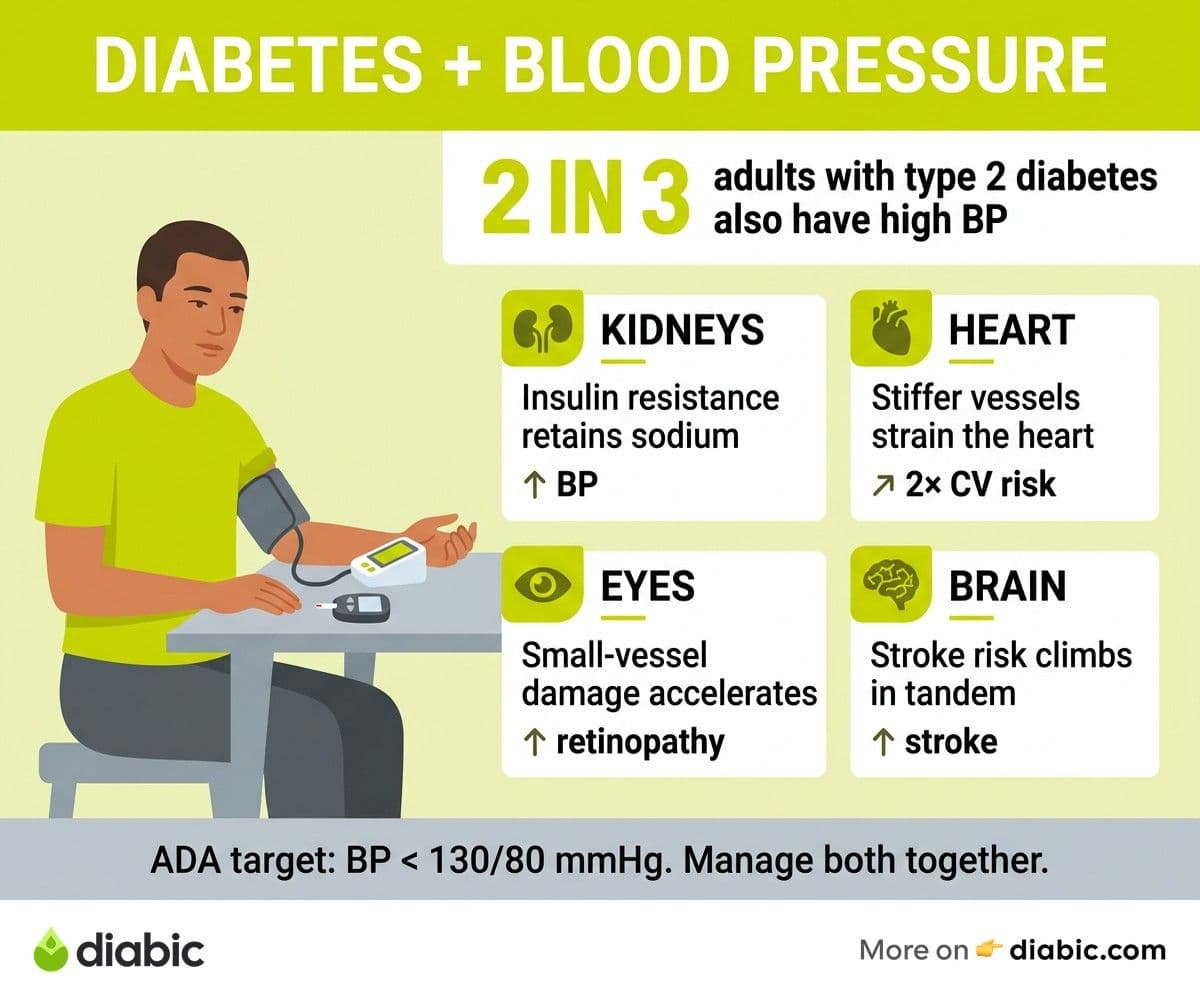
The two conditions share so much biology that researchers often refer to them as cousins. According to the American Diabetes Association Standards of Care, about two out of three adults with type 2 diabetes also have high blood pressure. This is not coincidence. Both conditions are driven by overlapping risk factors and similar damage to blood vessels.
The shared risk factors include excess body weight, low physical activity, diets heavy in processed food and sodium, chronic stress, poor sleep, and genetics. Each of these affects how your body uses insulin and how flexible your blood vessels remain over time.
Insulin resistance plays a central role. When cells stop responding well to insulin, your pancreas pushes out more of it. Higher circulating insulin levels signal the kidneys to retain sodium and water, which raises blood pressure. Chronic high blood sugar also damages the inner lining of blood vessels (the endothelium), making them stiffer and less able to dilate. Stiff vessels mean higher pressure to push the same amount of blood through.
The relationship runs both ways. High blood pressure damages the small vessels in your kidneys, eyes, and pancreas, which in turn worsens insulin resistance and blood sugar control. Each condition makes the other harder to manage, which is exactly what makes the pair so dangerous when ignored. We cover the deeper mechanism in our piece on how diabetes causes high blood pressure.
How Do Blood Pressure and Diabetes Affect Each Other?
The damage diabetes causes to blood vessel walls makes them more vulnerable to the mechanical stress of high blood pressure. Picture a garden hose. A clean, flexible hose can handle high water pressure with no trouble. The same hose, brittle from years of sun exposure, splits and leaks under the same pressure. Your blood vessels behave similarly.
Chronic hyperglycemia (high blood sugar) does several things to vessels:
- Glycation of proteins in the vessel wall makes them less elastic.
- Inflammation from glucose spikes makes the inner lining "stickier" for cholesterol and clotting factors.
- Oxidative stress damages the endothelium and reduces the production of nitric oxide, a molecule that helps vessels relax.
When you add high blood pressure on top of all this, the damage accelerates. Plaque builds up faster. Vessels narrow further. The heart has to work harder to push blood through, and the smallest vessels (in the eyes, kidneys, and feet) are hit hardest because they have the least margin for error.
From my experience: when I was first diagnosed with type 1 diabetes 14 years ago, no one mentioned blood pressure to me for years. I assumed glucose was the only number that mattered. The reality is that the blood pressure diabetes pairing is what determines long-term outcomes for most people with diabetes, and getting comfortable with home BP monitoring early changed how I think about my health every day.
The Combined Risk to Your Health
The reason providers push so hard on managing both conditions is that the cardiovascular numbers are striking. The landmark UK Prospective Diabetes Study (UKPDS) found that for every 10 mm Hg drop in systolic blood pressure in people with type 2 diabetes, there was a roughly 12 percent reduction in any diabetes-related complication and a 15 percent reduction in deaths related to diabetes. The combined statement from the American Heart Association and the ADA on cardiovascular disease and diabetes reinforces that managing both is more effective than focusing on either alone.
The specific complications worsened by the combination include:
- Heart disease and stroke: People with both conditions have roughly four times the risk of cardiovascular events compared to those with neither.
- Kidney damage (diabetic nephropathy): High blood pressure is the single biggest accelerator of kidney decline in people with diabetes. The two together can take kidneys from healthy to needing dialysis over a span of years.
- Eye damage (diabetic retinopathy): High blood pressure speeds the progression of retinopathy and increases the risk of bleeding in the retina.
- Peripheral artery disease: Reduced circulation in the legs and feet, which raises the risk of foot ulcers and amputation.
For more on heart-specific risks, our guide to reducing your diabetes heart attack risk covers the practical side of cardiovascular protection.
The flip side is encouraging. Because the two conditions are so closely linked, addressing both at once produces compounding benefits. The same lifestyle changes that lower blood pressure tend to improve blood sugar, and many medications prescribed for one condition help the other.
How Diabetes Causes High Blood Pressure
Several mechanisms link diabetes to elevated blood pressure. Insulin resistance is the headline player, but it works through several pathways. The CDC's overview of diabetes and high blood pressure summarizes the connection at a high level, but the biology is worth understanding.
First, insulin signals the kidneys to hold onto sodium. In a healthy state this is finely balanced. With insulin resistance, your body produces more insulin, which means more sodium retention, which means more fluid in the blood vessels and higher pressure. Second, chronic high blood sugar produces advanced glycation end products (AGEs) that stiffen the walls of arteries, reducing their ability to expand and contract with each heartbeat.
Third, diabetes is associated with increased activity in the sympathetic nervous system (the "fight or flight" branch). This raises heart rate and constricts vessels, both of which push blood pressure up. Finally, chronic inflammation, which is elevated in diabetes, damages the endothelium and reduces nitric oxide production. Nitric oxide is what allows your vessels to relax. Less of it means higher pressure.
These mechanisms reinforce each other. None of them require advanced kidney disease or any other complication. They begin in the years leading up to a diabetes diagnosis and continue throughout life with the condition.
Managing Both Conditions Together
A coordinated treatment plan matters more than treating each condition in isolation. The ADA suggests a blood pressure target of less than 130/80 mm Hg for most adults with diabetes, though your provider may set a different target based on your overall risk profile. We dig into specifics in our piece on ideal blood pressure numbers for diabetes.
Lifestyle changes do double duty here. The DASH eating pattern (Dietary Approaches to Stop Hypertension) reduces blood pressure and improves blood sugar simultaneously. Regular aerobic exercise improves both. Modest weight loss (5 to 10 percent of body weight) often produces meaningful improvements in both numbers. Reducing sodium to under 2,300 mg per day, cutting back on alcohol, and getting consistent sleep all support both conditions at once.
Medications also overlap helpfully. ACE inhibitors and ARBs (angiotensin receptor blockers) are often first-choice blood pressure medications for people with diabetes because they protect the kidneys in addition to lowering pressure. Some newer diabetes medications, including SGLT2 inhibitors and GLP-1 receptor agonists, modestly lower blood pressure as a side benefit. When considering medications, your provider will weigh interactions and side effects together rather than treating each prescription separately.
The key principle is simple: every appointment, every lab, and every change should consider both conditions. Treating one in a vacuum often misses the bigger picture.
Building Your Healthcare Team
Managing both conditions usually involves a few different providers. Your primary care physician or endocrinologist coordinates the overall plan and prescribes most medications. A diabetes educator (CDCES) or registered dietitian helps with practical lifestyle change. An ophthalmologist watches your eyes annually. A nephrologist may be involved if your kidney function is declining.
Monitoring frequency depends on your numbers. For blood pressure, most adults benefit from checking at home a few times a week, with formal readings at appointments every 3 to 6 months. The American Heart Association's guidance on home blood pressure monitoring explains how to do this accurately. For blood sugar, daily monitoring or continuous glucose monitoring is standard for many people with diabetes, with A1C tested every 3 to 6 months.
Useful questions to bring to appointments include:
- What is my current blood pressure target, and why that number?
- How are my kidneys doing? What is my eGFR and urine albumin?
- Are any of my medications doing double duty for both conditions?
- What is one change I could make this month that would help both numbers?
Asking questions like these signals to your provider that you want to participate in the plan, which usually leads to a better partnership and more useful answers.
Frequently Asked Questions
Why are blood pressure and diabetes connected?
Both conditions share risk factors and biological pathways. Insulin resistance leads the kidneys to retain sodium and damages blood vessel walls, while high blood sugar promotes inflammation that raises blood pressure further. Each condition worsens the other when left unaddressed, which is why providers treat the blood pressure diabetes pair as one connected problem.
How do blood pressure and diabetes affect each other?
High blood sugar damages the inner lining of blood vessels, making them more susceptible to the mechanical stress of high blood pressure. In turn, high blood pressure accelerates kidney, eye, and heart complications that diabetes already raises the risk for. The combination roughly quadruples cardiovascular risk compared to having neither condition, but managing both produces compounding benefits.
Can lifestyle changes alone manage blood pressure and diabetes?
For some people, especially those in the early stages of either condition, sustained lifestyle changes can bring both numbers into a healthy range. For many others, lifestyle changes work best alongside medication. Either way, regular movement, a Mediterranean or DASH-style diet, modest weight loss, sodium reduction, and good sleep are the foundation that everything else builds on.
If you want to keep going, our guide to ideal blood pressure numbers for diabetes is the natural next step. The reason we keep emphasizing the blood pressure diabetes connection is simple: small, consistent attention to both pays off more than dramatic effort on either one alone.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.