How Diabetes Causes High Blood Pressure
Understand how diabetes causes high blood pressure through insulin resistance, vessel stiffness, and kidney effects, and how to protect yourself.

In this article(11)
Understanding how diabetes causes high blood pressure helps explain why so many people with diabetes also deal with hypertension. The connection is not just coincidence but involves specific biological mechanisms that link blood sugar problems to blood vessel damage. Here is what happens inside your body when these two conditions converge.
Roughly two in three adults with diabetes also have hypertension, according to the American Diabetes Association. The overlap is so common that providers screen for one whenever they diagnose the other. The reason runs deeper than shared lifestyle factors. The biology of diabetes actively pushes blood pressure up.
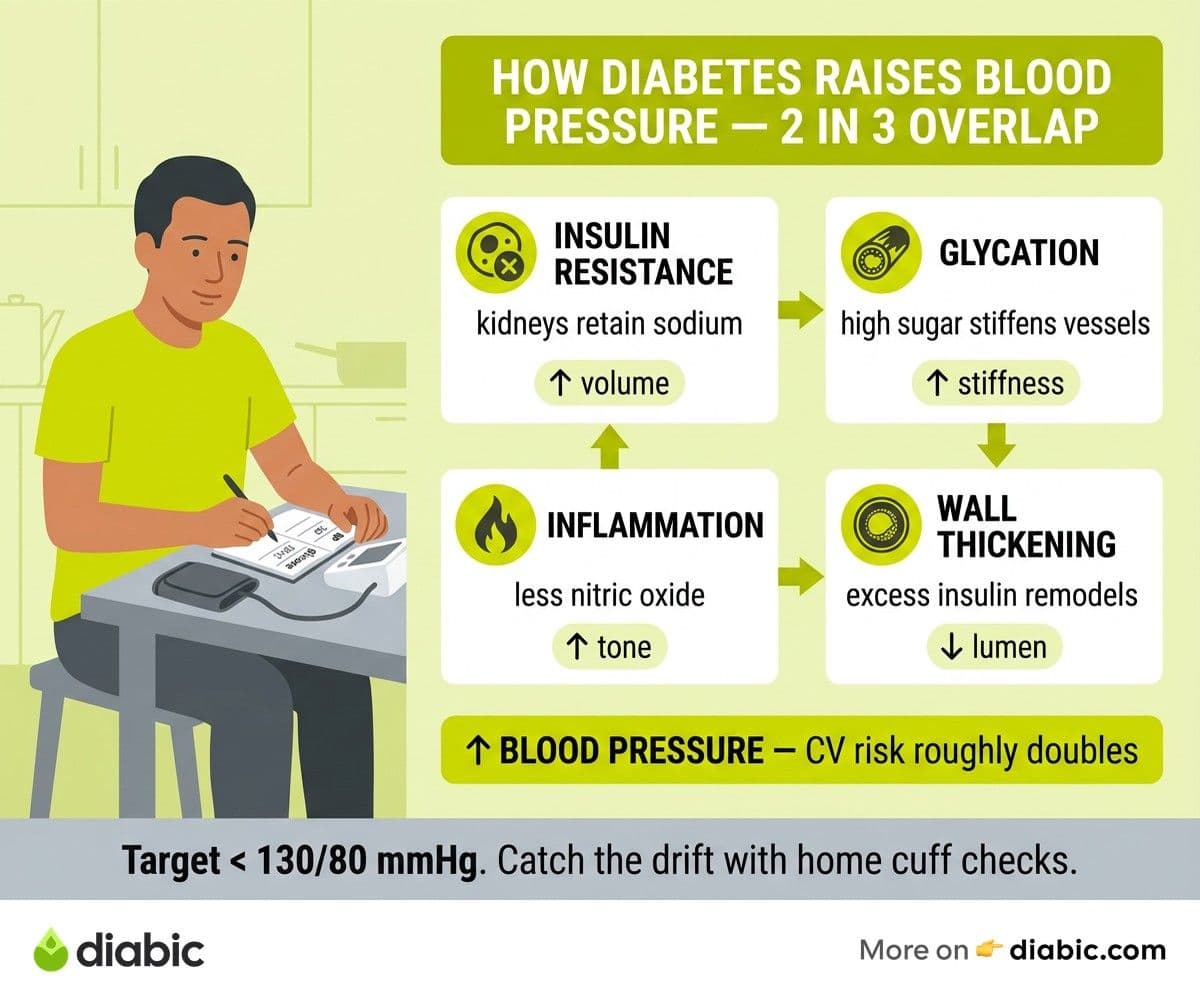
How Diabetes Causes High Blood Pressure: Four Mechanisms
Several mechanisms work together to drive the link. The first is sodium retention. Insulin signals the kidneys to hold onto salt, and when cells become resistant to insulin, the body produces more of it to compensate. Higher circulating insulin keeps the kidneys reabsorbing sodium they would otherwise excrete. More sodium means more fluid volume in the bloodstream, which raises pressure on artery walls.
Chronic high blood sugar adds a second layer. Glucose binds to proteins in the lining of blood vessels through a process called glycation. Over years, this stiffens the arteries and reduces their ability to expand and contract with each heartbeat. Stiffer vessels handle blood flow worse, and pressure climbs as a result.
Inflammation and oxidative stress make things worse. Persistent hyperglycemia damages the endothelium, the thin cellular layer inside blood vessels that controls how they relax. Inflamed, damaged endothelium produces less nitric oxide and more constricting signals. Vessels stay tighter than they should.
The fourth mechanism is more subtle. Excess insulin itself promotes thickening of the smooth muscle inside arterial walls. Thicker, narrower arteries push pressure up even when fluid volume is normal. This is one reason people with insulin resistance often develop hypertension years before their fasting glucose crosses the diabetes threshold. Research published in Diabetes Care has documented these pathways across decades of clinical studies.
The Biology Behind Blood Pressure and Diabetes
Two systems sit at the heart of the blood pressure diabetes connection: nitric oxide signaling and the renin-angiotensin-aldosterone system (RAAS).
Healthy endothelial cells produce nitric oxide, a small molecule that signals blood vessel walls to relax. Insulin normally boosts nitric oxide production. In insulin resistance, this signal weakens. Vessels stay constricted longer, and pressure inside them rises.
The RAAS is the body's main blood pressure thermostat. When the kidneys detect low pressure, they release renin, triggering a cascade that produces angiotensin II (a potent vasoconstrictor) and aldosterone (a hormone that holds onto sodium and water). In diabetes, this system runs hotter than it should. The pancreas, kidneys, and fat tissue all release more components of the cascade, even when blood pressure does not need raising.
The kidneys are where these systems collide. Diabetes damages the tiny filtering units called glomeruli, gradually reducing the kidneys' ability to balance fluid and salt. Damaged kidneys also release more renin, pushing the RAAS further. The result is a feedback loop: high blood sugar damages kidneys, damaged kidneys raise blood pressure, and high blood pressure damages the kidneys further.
High Blood Pressure and Diabetes: The Compounding Effect
When high blood pressure and diabetes occur together, the damage to blood vessels accelerates. The combination is not additive but multiplicative. Hypertension stresses already-fragile diabetic blood vessels in the eyes, kidneys, heart, and brain.
Cardiovascular disease risk roughly doubles when both conditions are present compared to either alone. The American Heart Association notes that the leading cause of death in adults with type 2 diabetes is cardiovascular disease, and uncontrolled blood pressure is one of the strongest drivers. Heart attack and stroke risk both climb in tandem with rising systolic numbers.
Treating both at the same time is not optional. Lowering blood pressure even modestly (by 10 mmHg systolic) can reduce major cardiovascular events by about 20 percent in adults with diabetes. The benefits compound over years. Our overview of why blood pressure and diabetes both matter explains the integrated approach providers take when both conditions show up together.
From my experience: After more than a decade of managing diabetes, I learned the hard way that blood pressure can creep up quietly while you focus on glucose. My fasting numbers were great for years before my BP started drifting. Adding regular cuff checks at home caught the change early enough to fix with lifestyle and one low-dose medication.
Can Controlling Diabetes Lower Blood Pressure?
Better blood sugar management does help. When A1C drops, vascular inflammation falls, glycation slows, and the kidneys handle sodium better. Many people see modest improvements in blood pressure when they bring glucose into target range, especially if they also lose weight in the process.
The catch is that blood sugar improvement alone usually is not enough. By the time someone has measurable hypertension, the underlying vascular damage often persists even after glucose normalizes. Most adults with both conditions still need dedicated blood pressure treatment. The good news is that the medications used (especially ACE inhibitors and ARBs) protect the kidneys at the same time, slowing the diabetes complication that drives the pressure problem.
Lifestyle changes do double duty. The DASH eating pattern, regular activity, weight loss in the 5 to 10 percent range, lower sodium intake, and limited alcohol all improve both glucose and pressure. Medication adjustments work alongside, not instead of, these changes.
The Impact on Kidneys, Heart, and Eyes
The downstream damage from combined diabetes and hypertension shows up first in three places.
Kidneys. Diabetic nephropathy and hypertension feed each other. The NIDDK describes the slow loss of kidney function that follows years of dual damage. Annual UACR (urine albumin-to-creatinine ratio) and eGFR testing catch the decline early. Our deeper guide to how diabetes affects the kidneys walks through the progression.
Heart. Stiffened arteries force the heart to work harder to push blood. Over years, the left ventricle thickens (a condition called left ventricular hypertrophy), reducing the heart's ability to fill and pump efficiently. Heart failure and atrial fibrillation become more common. The diabetes heart attack risk climbs through both the arterial damage and the increased clotting tendency that comes with diabetes.
Eyes. Diabetic retinopathy progresses faster when blood pressure is uncontrolled. The fragile new blood vessels that grow in proliferative retinopathy are more likely to bleed under high pressure. Annual dilated eye exams catch problems early, often before vision changes appear.
Protecting Yourself When You Have Both Conditions
The protection strategy looks the same whether you started with diabetes or hypertension first. Three commitments matter most.
Monitor regularly. Home blood pressure cuffs are inexpensive and accurate. Aim for readings twice a day for a week before each checkup, then take averages. Track them in a notebook or app. CGM or daily fingersticks plus quarterly A1C give the same kind of trend data for glucose.
Address root causes. The DASH eating pattern, post-meal walks, weight loss in the 5 to 7 percent range, sodium under 2,300 mg per day, and stress reduction all help both numbers. Our piece on natural ways to lower blood pressure covers the daily moves that compound over months.
Build a unified treatment plan. Ask your provider whether your blood pressure medications are kidney-protective (ACE inhibitors and ARBs are first-line for adults with diabetes per ADA guidelines). Ask whether your diabetes medications have cardiovascular benefits (SGLT2 inhibitors and GLP-1 agonists do). The same prescription often addresses both conditions.
FAQ
Why does diabetes cause high blood pressure?
Diabetes causes high blood pressure through multiple mechanisms: insulin resistance promotes sodium retention by the kidneys, chronic high blood sugar stiffens blood vessel walls, and inflammation damages the cells lining blood vessels. These processes make blood pressure harder to regulate, which is why so many people with diabetes also develop hypertension within a few years of diagnosis.
Can controlling diabetes lower blood pressure?
Improved blood sugar management can have a positive effect on blood pressure, but most people with both conditions still need dedicated blood pressure treatment. Better glucose control reduces the vascular damage that drives hypertension, but established high blood pressure usually requires its own therapy alongside diabetes care.
What is the blood pressure target for diabetes?
The ADA recommends a target below 130/80 mmHg for most adults with diabetes. Some patients (especially those with high cardiovascular risk) may benefit from even lower targets. Your provider will set a specific goal based on your age, kidney function, and other risk factors.
Does insulin itself raise blood pressure?
Excess circulating insulin (common in insulin resistance and type 2 diabetes) can promote sodium retention and arterial wall thickening, both of which raise pressure. Prescribed insulin therapy at appropriate doses is not the same problem; the issue is chronically elevated insulin from underlying resistance, not therapeutic use.
When you understand how diabetes causes high blood pressure, the case for treating both at the same time becomes obvious. The two conditions share roots, share damage pathways, and respond to many of the same lifestyle changes. Catching the link early gives you the best shot at protecting your kidneys, heart, and eyes for the long haul.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.