Generic vs Brand Insulin: Is There a Difference?
Generic vs brand insulin compared: how biosimilars are approved, what you save with Semglee or ReliOn, and how to talk to your doctor about switching.

In this article(11)
The pharmacist hands you a box that looks almost like the one you have used for years, except the label is different and the price tag is half. The generic vs brand insulin question follows that moment for a lot of people, and the answer is more interesting than a yes or no. Biosimilar insulins have entered the United States market in the last several years, and for most people they offer the same clinical effect at a meaningfully lower cost.
We want to be precise here, because language matters when your safety depends on it. A true small-molecule generic, like generic ibuprofen, is chemically identical to the brand. Insulin is a large protein produced in living cells, which is why its lower-cost versions are technically biosimilars or follow-on biologics rather than generics in the traditional sense. The practical takeaway is that biosimilars are highly similar to the originator insulin and meet rigorous regulatory standards, but the regulatory pathway is different.
In this guide, we walk through what biosimilar approval looks like, which lower-cost options are on shelves now, where Walmart insulin fits in, and how to have a productive conversation with your doctor if you want to switch. We are not going to tell you what to take, but we will give you the vocabulary and the context to decide alongside your care team.
From my experience: I switched from Lantus to Semglee around 2022 after my insurance moved it to a preferred tier, and the only difference I noticed was the box. My fasting numbers in the first ten days sat in the same low-100s range I was used to, and my next A1C looked like the previous one. The pharmacist did warn me the pen click felt slightly different, which turned out to be true but inconsequential.
Generic vs Brand Insulin: Understanding the Basics
When you hear "generic" at the pharmacy counter, the word can mean two very different things in the insulin world. For small-molecule drugs, the FDA approves generics that are chemically identical to the brand and shows the same absorption in the body. Insulin does not work that way because each molecule is a complex protein, and "identical" is impossible to confirm at that scale. The FDA created a separate pathway, the biosimilar pathway, to handle this difference.
A biosimilar must show no clinically meaningful differences from its reference product in safety, purity, and potency. The FDA biosimilar information page explains that biosimilars undergo extensive analytical, animal, and human studies, including comparative pharmacokinetic and pharmacodynamic trials. A biosimilar can also earn an "interchangeable" designation, which means a pharmacist can substitute it for the reference product without prescriber intervention, subject to state law.
Insulin biosimilars took longer to reach the United States than other countries, partly for regulatory reasons. Until 2020, insulin was approved as a drug rather than a biologic, which kept it outside the biosimilar pathway. The transition that year reclassified insulin as a biologic and opened the door to biosimilar competition. The NIDDK overview of insulin therapy provides clinical context on how the different insulin categories are used.
Standards that biosimilar insulins must meet include comparative clinical studies in people with diabetes, post-market surveillance, and ongoing manufacturing controls. None of this is a paperwork shortcut, and the development cost of a biosimilar runs into the hundreds of millions of dollars. The savings to patients come from competition, not from cutting corners on quality.
Affordable Insulin Options: Generic Choices Available Now
Several biosimilar and follow-on insulins are now available, and the list is growing. Semglee, a biosimilar to Lantus (insulin glargine), was the first interchangeable biosimilar insulin approved in the United States and reached pharmacies in 2021. It is available in vials and pens, and pharmacists in most states can substitute it for Lantus without contacting the prescriber, similar to how generic substitution works for traditional medications.
Insulin lispro from Sanofi and other manufacturers serves as a follow-on to Humalog. Pricing for these unbranded versions often runs forty to sixty percent below their reference products, and the chemistry is the same insulin lispro molecule. Eli Lilly also markets an authorized generic of Humalog, which is the same product as the brand made by the same company under a different label and a lower price. Authorized generics are not biosimilars, but they hit the same goal of lowering out-of-pocket cost.
ReliOn insulin at Walmart is a different category, and we cover it in detail below because it deserves its own section. The pipeline for biosimilar insulins is also active. The ADA position statement on biosimilar insulin discusses both current and emerging products and explains why the organization supports broader biosimilar uptake as a way to expand access.
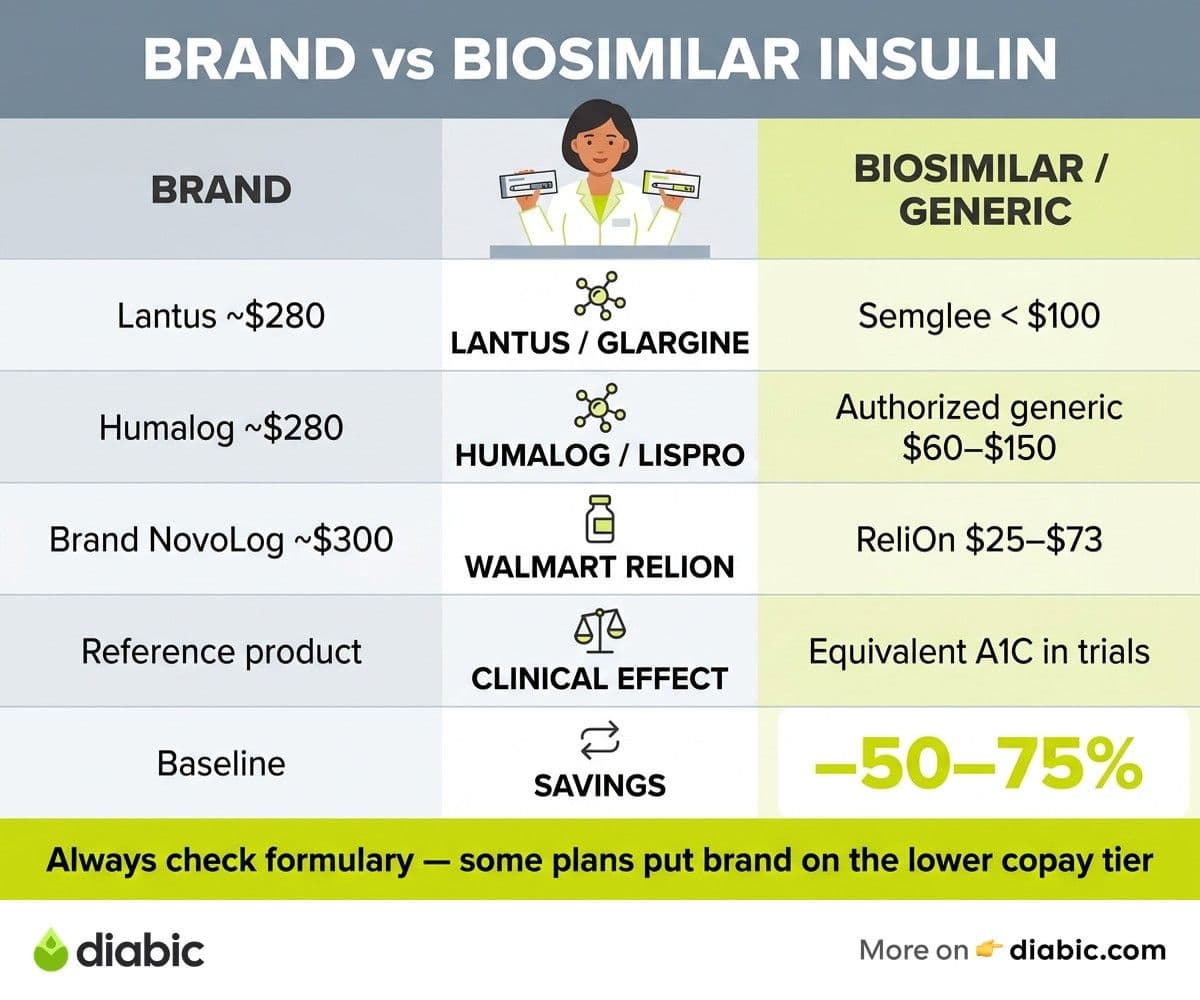
Here is how the most common brand and lower-cost options stack up at a glance:
Cash prices move around, but the pattern holds: biosimilars and authorized generics consistently undercut their reference brands without changing the underlying molecule.
Price comparisons help make the abstract concrete. Without insurance, a single vial of Lantus often runs around two hundred eighty to three hundred dollars, while Semglee from manufacturer cash programs can fall under one hundred dollars. Humalog runs roughly the same as Lantus at retail, while authorized generic insulin lispro can come in at sixty to one hundred fifty dollars per vial. With insurance, the spread depends entirely on your plan's formulary, which we get into in the cost section. We also cover the broader landscape in our guide to affordable insulin options and where to find them.
Walmart Insulin: A Special Case
Walmart's ReliOn line is its own conversation because it includes both older human insulins and a newer biosimilar. ReliOn NPH and ReliOn Regular are human insulins, the same formulations that were the standard of care in the 1980s and 1990s before rapid-acting and long-acting analogs arrived. They are sold over the counter in most states and cost roughly twenty-five dollars per vial.
Walmart also carries ReliOn NovoLog (insulin aspart), a rapid-acting analog at a discounted price, typically around seventy-five dollars per vial. This is a branded insulin sold under a private-label arrangement rather than a biosimilar, but the pricing is meaningfully below standard NovoLog. For people without insurance who use rapid-acting insulin, this single option can change the monthly math considerably.
How human insulin differs from modern analogs matters a lot for safety. NPH insulin peaks roughly four to six hours after injection and has a less predictable profile than insulin glargine or detemir, which means meal timing and snack patterns become more rigid. Regular insulin acts more slowly than rapid-acting analogs, which means injecting thirty minutes before a meal rather than at the table. People who switch from analogs to human insulin without dose and timing adjustments can experience hypoglycemia or post-meal highs.
Who can safely use Walmart insulin and who should avoid it is a question for your care team, not a search engine. People with stable Type 2 diabetes on a simple regimen, who are running out of insulin and cannot afford their prescribed product this month, can sometimes bridge with ReliOn human insulin under their provider's direction. People with Type 1 diabetes, frequent hypoglycemia, or pump therapy should generally not switch to NPH or Regular without close medical supervision, because the timing differences can be dangerous. We get into more nuance in our piece on Walmart insulin options explained, but the headline is that affordable does not always mean appropriate.
Effectiveness and Safety: What the Data Shows
Clinical trial data comparing biosimilars to their reference products is now substantial. For Semglee, the INSTRIDE 1 and INSTRIDE 2 trials enrolled hundreds of participants with Type 1 and Type 2 diabetes and showed equivalent A1C reductions, similar hypoglycemia rates, and comparable injection-site reactions versus Lantus. The Endocrine Society biosimilar insulin clinical guidance summarizes how these trials are designed and why their results support clinical equivalence.
Real-world outcomes studies have followed. Several large database analyses have tracked patients who switched from Lantus to Semglee or from Humalog to insulin lispro and found no meaningful difference in A1C trajectories, hypoglycemia rates, or hospital visits. Pharmacy benefit managers have used these data to move biosimilars to preferred tiers, sometimes faster than the average patient experience would suggest is comfortable, which is a separate concern about formulary mechanics.
FDA post-market surveillance continues to monitor biosimilar insulins after approval. The agency requires manufacturers to submit periodic safety updates, and pharmacovigilance teams track adverse events through MedWatch reports. To date, post-market data has not surfaced safety differences between approved biosimilar insulins and their reference products. That is a strong signal, though not a guarantee, that the products perform the same way for most users.
What endocrinologists say in clinical practice is more nuanced than the trial data alone. Most are comfortable switching patients to biosimilars, particularly Semglee, because the evidence is solid and the cost savings are real. Some prefer to keep individual patients on the originator if they are achieving target A1Cs without complications, simply to avoid disrupting a working regimen. The conversation is rarely about whether biosimilars work, and almost always about whether the timing of a switch makes sense for a specific person.
The Cost Factor: How Much Can You Save
Average savings when switching from brand to biosimilar depend on whether you have insurance, what kind, and where you live. For people paying cash, switching from Lantus to Semglee can save roughly one hundred fifty to two hundred dollars per vial. Switching from Humalog to authorized generic insulin lispro can save eighty to one hundred fifty dollars per vial. Annual savings in the low thousands are not unusual for people on basal-bolus regimens.
Insurance formulary considerations can flip the math in either direction. Some plans put biosimilars on a lower copay tier than the brand, which makes the switch obvious. Other plans, often through deals with the originator manufacturer, keep the brand on a preferred tier and price the biosimilar higher. Always check your plan formulary before you switch, because the pharmacy counter is not the place to discover that the biosimilar costs more out of pocket on your specific plan. We dig into the broader picture in the real cost of diabetes management.
Out-of-pocket costs without insurance look very different from costs with insurance. Manufacturer cash-pay programs from Eli Lilly and Sanofi cap insulin at thirty-five dollars per vial or pen for people who qualify, regardless of insulin brand. These programs can sometimes beat both biosimilar cash prices and insurance copays, so they are worth checking before you commit to a switch.
When brand insulin actually costs less than biosimilar, you are usually looking at a formulary quirk. A pharmacy benefit manager might receive larger rebates from the originator manufacturer and pass some of that on as a lower copay. The list price of the brand stays high, the rebate stays invisible, and you experience a cheaper copay on the brand than on the biosimilar. According to IQVIA Institute research on biosimilar uptake, this dynamic has slowed biosimilar adoption in some markets even when the underlying economics favor switching.
How to Talk to Your Doctor About Switching
The conversation goes better when you bring specific questions. Asking your prescriber whether a biosimilar exists for your current insulin, whether your plan covers it on a lower tier, and whether interchangeable substitution applies in your state covers most of what matters. If your provider is hesitant, ask which clinical concerns drive that, because sometimes the answer is a recent A1C trend they want to stabilize before changing variables.
Monitoring your blood sugar during the transition is the same kind of attention you would give any change in your regimen. Most people do not notice any difference after switching from Lantus to Semglee or Humalog to insulin lispro, which is the result the clinical trials predicted. A small number of people experience minor differences in absorption that show up as slightly higher or lower glucose readings in the first week or two. Logging your numbers a bit more carefully during the first ten days gives you and your care team useful data.
What to expect in the first few weeks is mostly nothing dramatic. The injection routine, the storage rules, the timing, and the units stay the same. The packaging looks different, the price looks different, and your A1C three months later usually looks the same as it would have on the originator. If you notice anything unusual, like persistent highs at the same dose or new injection-site reactions, call your prescriber rather than waiting for your next appointment.
When switching is not recommended, your provider will tell you. People with brittle Type 1 diabetes, frequent hypoglycemia unawareness, pregnancy, or a history of allergic reactions to specific formulations may have reasons to stay on a specific product. Pump users have additional considerations because not every pump manufacturer has tested compatibility with every insulin. None of this is a reason to assume biosimilars are inferior, just a reason to make the decision in partnership with your care team.
FAQ
Is generic insulin as good as brand name?
Yes. FDA-approved biosimilar insulins have showed the same safety, purity, and potency as their reference products in head-to-head clinical trials, and post-market surveillance has not identified meaningful safety differences. They undergo extensive analytical and clinical testing before approval and ongoing monitoring after approval. The word "generic" is technically inaccurate for insulin, since the regulatory category is biosimilar, but the practical clinical effect is highly similar.
Should you switch to generic insulin?
If cost is creating a barrier to consistent insulin use, switching to a biosimilar can save meaningful money without sacrificing quality for most people. The decision is best made with your prescriber, who can recommend a specific biosimilar that matches your current insulin and help you monitor blood sugar during the first weeks. People with very tight control, complex regimens, or pump therapy may need additional planning, but the underlying products are clinically equivalent to their reference insulins.
What is the difference between Semglee and Lantus?
Semglee is a biosimilar to Lantus, meaning it is highly similar to Lantus in safety, purity, and potency. Both are insulin glargine, both are dosed once daily for most people, and both have flat twenty-four-hour action profiles. The main differences are the manufacturer and the price, with Semglee available at a substantially lower cost. Semglee is also designated as interchangeable, which means pharmacists in most states can substitute it for Lantus without contacting the prescriber.
Can I use Walmart insulin instead of my prescription?
Sometimes, but only in close coordination with your healthcare provider. Walmart's ReliOn human insulins (NPH and Regular) act differently from modern analog insulins, and switching without dose and timing adjustments can cause hypoglycemia or post-meal highs. Walmart also sells ReliOn NovoLog, a discounted analog that behaves like prescription NovoLog. If you are facing an affordability problem, call your provider before making a switch so they can help you do it safely.
The bottom line on generic vs brand insulin is that biosimilars give most people the same clinical effect at a meaningfully lower cost, and the regulatory standards behind them are rigorous rather than relaxed. Bring the question to your next appointment with one specific ask, whether your current insulin has an FDA-approved biosimilar that fits your plan, and use the first few weeks of any switch to log your numbers a little more carefully. Compare the cash price, the copay, and any manufacturer assistance program before you commit, because the cheapest path varies by plan. The generic vs brand insulin decision is rarely about whether the products work the same. It is about which combination of price, coverage, and routine makes diabetes care sustainable for you this year.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Living with Diabetes
View all
Patient Assistance Programs for Diabetes Medication
Patient assistance programs diabetes patients qualify for can cut prescription costs to little or nothing. Here is how to find and apply for them.

Diabetes Supply Savings Tips That Actually Work in Real Life
Practical diabetes supply savings tips for cutting costs on test strips, CGMs, insulin, and pump supplies without compromising your care.
Diabetes Supply Savings Tips That Actually Work in Real Life
Practical diabetes supply savings tips for cutting costs on test strips, CGMs, insulin, and pump supplies without compromising your care.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.