Alcohol and Type 2 Diabetes: Risks and Limits
Alcohol and type 2 diabetes interact in ways most articles skip. Learn the real risks, ADA limits, medication interactions, and how to drink more safely.

In this article(10)
The conversation about alcohol and type 2 diabetes is full of mixed signals. One headline says a glass of red wine may protect the heart, the next warns that alcohol pushes blood sugar in unpredictable directions and feeds the very inflammation behind insulin resistance. Both can be true at the same time, which is exactly why the topic feels so confusing.
Sorting fact from wishful thinking matters when your blood sugar management is already a daily project. Drinking with type 2 diabetes is not automatically off limits, but it is also not as simple as "moderate is fine." The risks shift based on which medications you take, how your liver is doing, what you eat alongside the drink, and how your body has responded historically.
This guide walks through the real interactions, the safer-drinking limits suggested by the American Diabetes Association, and the situations where skipping a drink is the smarter call. We will keep the language plain and the recommendations practical.
How Alcohol and Type 2 Diabetes Interact
Alcohol and type 2 diabetes share the same metabolic stage, and they tend to elbow each other for space. The liver is the main reason. When you drink, your liver puts most other tasks on hold to break down ethanol, and one of those paused tasks is releasing glucose into the bloodstream between meals. For someone whose blood sugar is already running high, that pause can briefly look like a benefit. For someone on insulin or a sulfonylurea, it can become a hypoglycemia event hours after the last sip.
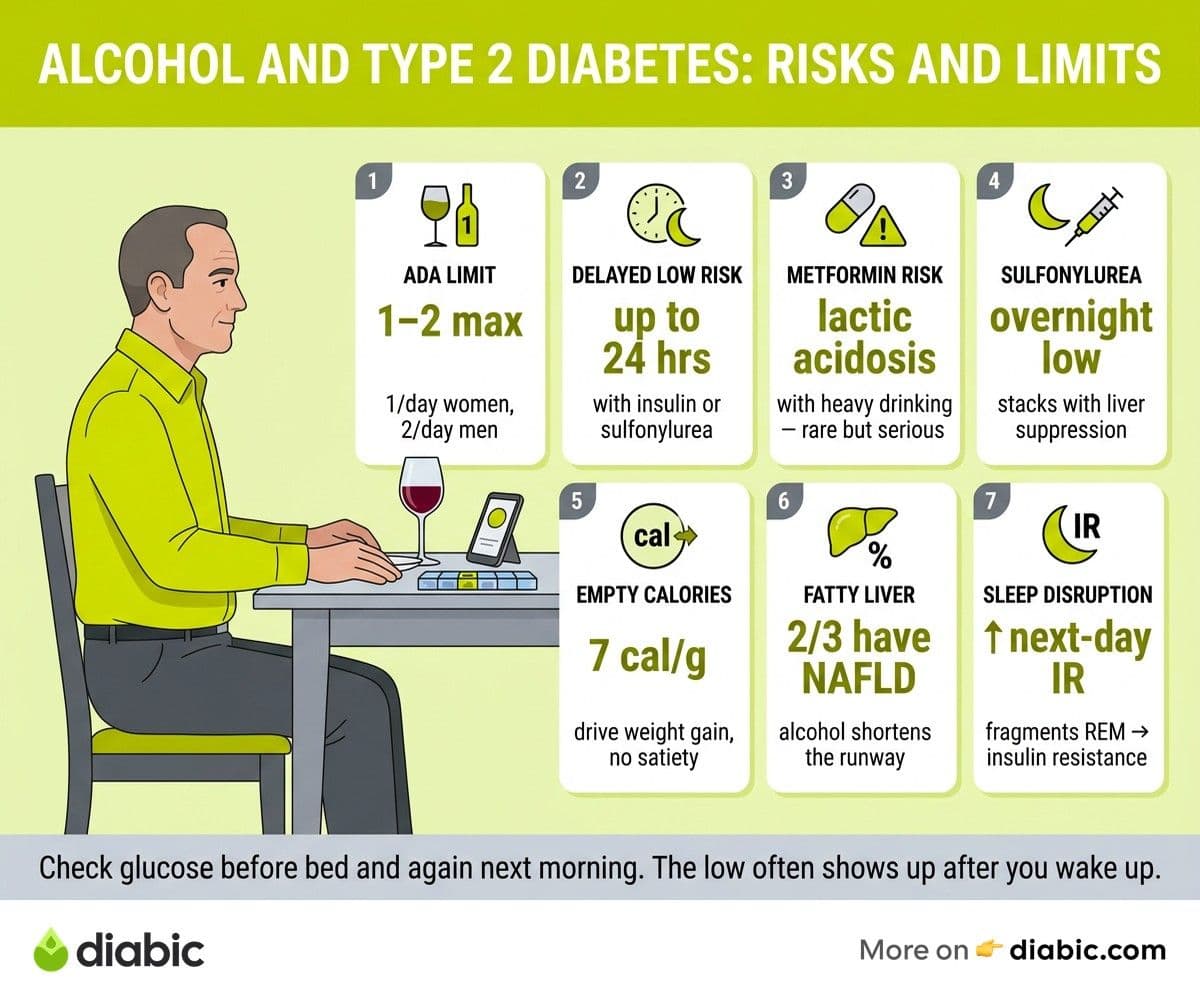
Alcohol also interacts with insulin sensitivity, but the relationship is dose dependent. Light to moderate intake has been associated in some observational studies with slightly improved insulin sensitivity, while heavier and more frequent drinking pushes the other direction and worsens insulin resistance over time. The Centers for Disease Control and Prevention defines moderate drinking as up to one drink per day for women and up to two for men, and that line is where most of the cardiovascular benefit research caps out.
Weight is the third lever. Alcohol carries roughly 7 calories per gram with no fiber, no protein, and very little nutritional return. Mixers and sweet cocktails stack carbs on top of those empty calories, which makes weight management harder and feeds the visceral fat that drives type 2 diabetes in the first place. A single craft cocktail can deliver 300 to 500 calories without registering as a meal in your memory.
Medications complicate the picture further. Metformin, when combined with heavy drinking, raises the rare but serious risk of lactic acidosis. Sulfonylureas like glipizide and glyburide stack their glucose-lowering action on top of alcohol's liver-suppression effect, which is the most common setup for severe overnight lows. Insulin behaves similarly. SGLT2 inhibitors and GLP-1 receptor agonists do not have the same dramatic interaction, but they can change appetite and hydration in ways that interact with drinking.
Risks of Alcohol Consumption with Type 2 Diabetes
Hypoglycemia is the headline risk and the one most often underestimated. The drop usually shows up several hours after the last drink, often during sleep, when you are least able to feel symptoms or reach for glucose. The National Institute on Alcohol Abuse and Alcoholism notes that alcohol can cause low blood sugar to last for up to 24 hours after drinking in people taking insulin or insulin secretagogues.
Liver health is the second concern. Type 2 diabetes is closely tied to non-alcoholic fatty liver disease, which now affects roughly two thirds of adults with the condition. Adding alcohol on top of an already stressed liver shortens the runway to fibrosis and cirrhosis. If your most recent labs flagged elevated liver enzymes, that is a direct conversation to have with your provider before drinking again.
Cardiovascular risk is more nuanced. Alcohol raises triglycerides, often substantially, and high triglycerides are an independent risk factor for heart disease. The American Heart Association notes that the supposed heart benefits of moderate drinking are increasingly questioned, especially given the parallel risks for blood pressure, atrial fibrillation, and certain cancers. For someone already managing type 2 diabetes, that risk-benefit calculation tilts toward caution rather than enthusiasm.
Blood pressure tends to climb with regular drinking, especially above the moderate threshold. Add the dehydration that follows a heavier night, and the next morning's blood pressure reading and blood sugar reading often both run higher than usual. Research published in the Diabetes Care journal has consistently linked heavier alcohol intake with worse glycemic outcomes in adults with type 2 diabetes.
Effects of Alcohol on Type 2 Diabetes Management
The disruption to blood sugar patterns can stretch well past the night you drank. Alcohol and type 2 diabetes effects often show up the next morning as a fasting reading that does not match what you ate the day before. Sometimes it runs higher because of the carbs in a cocktail, sometimes lower because of the lingering liver suppression, and sometimes it bounces unpredictably as the liver catches up.
Sleep is part of the chain. Even small amounts of alcohol fragment sleep architecture, particularly the second half of the night when REM sleep should dominate. Poor sleep is its own driver of insulin resistance, so the night you drink can quietly raise your blood sugar the next day even if your food choices stay the same. People wearing a continuous glucose monitor often see this pattern clearly for the first time.
Alcohol can also blur the warning signs of both highs and lows. The shaky hands, sweating, confusion, and irritability of hypoglycemia overlap heavily with how being drunk feels, both to you and to the people around you. Friends may interpret a dangerous low as "they had too much" and skip the very steps that would actually help. This is part of why glucose tablets and a clear plan with the people you are with matter more than they sound on paper.
Carb counting becomes harder too. A 12-ounce regular beer carries 12 to 15 grams of carbs, a 5-ounce glass of dry wine maybe 3 to 5 grams, and a margarita can run from 25 to over 50 grams depending on the recipe. None of these come with the protein and fiber that slow absorption, so the curve looks different on a CGM than the same carbs from a meal. If you keep a food log alongside your readings for a few weeks, you start to see how your specific body handles each drink type.
Type 2 Diabetes and Alcohol: Setting Safe Limits
The American Diabetes Association recommends that adults with type 2 diabetes who choose to drink follow the same general moderate-drinking limits as the broader population, which is up to one drink per day for women and up to two for men. A standard drink is defined as 12 ounces of regular beer, 5 ounces of wine, or 1.5 ounces of distilled spirits. These numbers do not stack across the week, so saving up for a Saturday night of seven drinks is not the same as one a day.
Several practical habits make those limits easier to honor. Eating before and during drinking is the single most protective move, because food slows alcohol absorption and gives your liver something other than ethanol to work on. Skipping the meal and ordering the drink first is the setup for a lot of late-night hypoglycemia stories.
Drink choice matters more than most people realize. Sugary mixers, dessert wines, and pre-batched cocktails can deliver 30 to 60 grams of carbs in a single glass, which can spike blood sugar even if you have planned for the alcohol itself. Our roundup of the best low-carb alcoholic drinks for diabetes walks through specific options. For a deeper look at the most-asked-about drink, our piece on how wine affects blood sugar levels breaks down dry versus sweet styles. And if you want a broader playbook, our guide to safe drinking with diabetes covers the full picture.
From my experience: After 14 years of living with type 1 diabetes, I have learned that the second drink is the one that almost always rewrites my next morning. The first drink, paired with a real meal, usually behaves predictably. The second one, especially after the food is cleared and the conversation is good, is where the overnight low or the surprise 11 a.m. spike sneaks in. Capping the night at one, ordering a glass of water alongside it, and checking my CGM before bed is the routine that has actually held up over years. The discipline is not glamorous, but it has saved me a lot of bad mornings.
Counting alcohol within your daily carb target is the next step. Many people lump alcohol in with carbs, which is conceptually fine but technically inaccurate. The cleaner approach is to budget the carbs from the mixer or the beer separately, and to remember that the alcohol itself can lower blood sugar later. Testing more often on drinking nights, including a check before bed and once during the night if you tend to run low, is how you catch the curve before it catches you.
Timing also matters. Drinking right after a workout, when muscle glycogen is depleted, raises hypoglycemia risk meaningfully. Drinking on a fasted morning is similar. Pairing alcohol with a meal that includes some protein, fat, and slow carbs gives your body the runway it needs.
When Drinking Is Not Worth the Risk
Some situations turn the risk-benefit calculation lopsided. Diabetic neuropathy is one of them. Alcohol is independently neurotoxic, and even moderate intake can worsen the burning, tingling, and numbness that already make daily life harder. If your provider has diagnosed peripheral or autonomic neuropathy, abstaining or drinking only rarely is the safer call.
Liver conditions move the needle even further. Fatty liver, hepatitis, elevated enzymes, or any history of pancreatitis all argue strongly against alcohol. The same goes for advanced kidney disease, where alcohol contributes to dehydration and electrolyte shifts the kidneys are already struggling with.
Medication interactions deserve specific mention. Sulfonylureas and insulin top the list for hypoglycemia risk. Metformin and alcohol together raise lactic acidosis risk, particularly during binge drinking episodes. Sleep medications, certain antidepressants, and opioid pain medications all multiply alcohol's effects in dangerous ways. The pharmacist who fills your prescriptions is a good source for a personalized review.
Problem drinking is its own category. The screening question most providers use is whether you have ever felt you should cut down, been annoyed by criticism of your drinking, felt guilty about it, or needed a drink first thing in the morning. Two or more "yes" answers warrants a real conversation. Type 2 diabetes makes alcohol use disorder harder on the body in ways that are not always visible until something breaks. The NIAAA's resources on rethinking drinking are a starting point if any of this lands close to home.
There is also the simpler answer of "not tonight." Skipping the drink at a wedding, a holiday meal, or a tough week is not deprivation, it is information. Many people find that after a month or two of not drinking, their fasting numbers improve, their sleep deepens, and their A1C trend changes in ways no medication adjustment had achieved. The decision to drink, like the decision to eat, is yours, and it does not have to be the same every time.
Frequently Asked Questions
How much alcohol can you drink with type 2 diabetes?
The ADA recommends no more than one drink per day for women and two for men, where a drink is 12 oz of beer, 5 oz of wine, or 1.5 oz of spirits. Your personal limit may be lower depending on your medications, liver health, weight goals, and how alcohol affects your blood sugar individually. A conversation with your provider about your specific situation is the safest starting point.
What are the risks of drinking alcohol with type 2 diabetes?
The main risks are hypoglycemia (especially with insulin or sulfonylureas), weight gain from empty calories, elevated triglycerides, worsened liver health, and impaired ability to recognize low blood sugar. Alcohol also disrupts sleep quality, which can raise next-day blood sugar even without a hangover. Heavier drinking compounds all of these and adds long-term cardiovascular and cancer risks.
Does alcohol raise or lower blood sugar in type 2 diabetes?
Both, depending on the drink and the timing. Sugary drinks, beer, and sweet cocktails tend to raise blood sugar in the short term because of their carb content. Pure alcohol like spirits or dry wine tends to lower blood sugar over the next 4 to 24 hours by suppressing the liver's glucose release. People on insulin or sulfonylureas feel the lowering effect more strongly.
Is red wine good for type 2 diabetes?
Some studies have suggested that moderate red wine intake may have small cardiovascular and antioxidant benefits, but newer research questions whether any amount of alcohol is truly beneficial. If you already enjoy a glass occasionally and your provider agrees it fits your health picture, dry red wine is among the lower-carb options. Starting to drink for health reasons alone is not recommended, and the rest of this guide on alcohol and type 2 diabetes covers why even moderate intake deserves a thoughtful conversation with your care team.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Living with Diabetes
View all
Generic vs Brand Insulin: Is There a Difference?
Generic vs brand insulin compared: how biosimilars are approved, what you save with Semglee or ReliOn, and how to talk to your doctor about switching.

Patient Assistance Programs for Diabetes Medication
Patient assistance programs diabetes patients qualify for can cut prescription costs to little or nothing. Here is how to find and apply for them.

Diabetes Supply Savings Tips That Actually Work in Real Life
Practical diabetes supply savings tips for cutting costs on test strips, CGMs, insulin, and pump supplies without compromising your care.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.