Thyroid Medication and Diabetes Interactions Guide
Thyroid medication diabetes interactions explained, plus the questions to ask your doctor about timing, dose changes, and TSH monitoring.

In this article(33)
If you are managing both a thyroid condition and diabetes, understanding thyroid medication diabetes interactions can help you avoid unexpected blood sugar changes and get the most from your treatment. The questions you bring to your next appointment matter more than you might think.
Thyroid drugs are some of the most prescribed medications in the world, and they generally have a long safety record. But once they meet insulin or oral diabetes medications, small interactions and timing details can have an outsized effect on blood sugar. This guide gives you the questions worth asking and the context to understand the answers.
Thyroid Medication Diabetes Interactions Explained
Most thyroid medications work by either replacing missing thyroid hormone or blocking an overactive gland. Either action shifts metabolism, and shifting metabolism shifts how your body handles glucose and insulin.
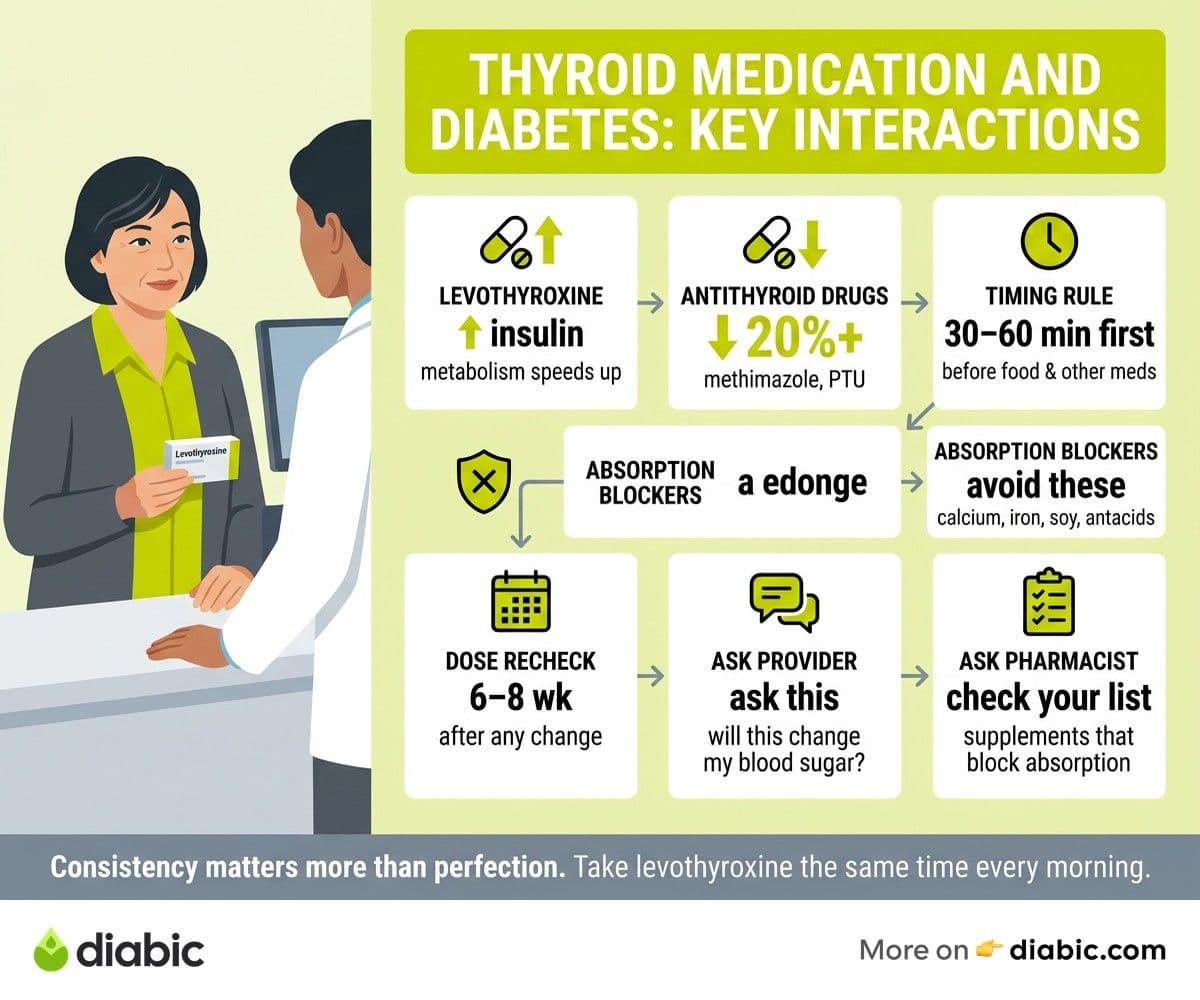
Levothyroxine, the most common thyroid hormone replacement, gradually returns metabolism to a normal rate. As that happens, glucose absorption speeds back up, the liver produces glucose more efficiently, and insulin clearance increases. The practical effect is that insulin requirements may rise modestly during the first few months on levothyroxine, especially when starting from a long period of untreated hypothyroidism.
Antithyroid drugs like methimazole and propylthiouracil (PTU) work in the opposite direction. They lower thyroid hormone production, which slows metabolism. People who start these drugs while in a thyrotoxic state often see insulin needs drop as glucose handling normalizes, sometimes by 20 percent or more.
Direct chemical interactions between thyroid drugs and diabetes drugs are relatively few. The bigger story is the indirect effect through metabolism. The American Thyroid Association outlines this dynamic and recommends careful monitoring during dose changes.
Timing Interactions
Levothyroxine absorption is sensitive to other medications and food. The standard advice is to take it 30 to 60 minutes before breakfast on an empty stomach, with water only. Coffee, calcium supplements, iron, and certain antacids can reduce absorption significantly.
Metformin, sulfonylureas, GLP-1 agonists, and insulin do not chemically interfere with levothyroxine, but timing still matters. Most people take their thyroid pill first thing in the morning and then their diabetes medications and breakfast 30 to 60 minutes later. This routine works well as long as it is consistent.
What Should people with diabetes Ask About Thyroid Medication
Coming to an appointment with specific questions makes the visit more productive. The list below covers the topics most likely to affect your day-to-day blood sugar and overall well-being.
Will This Medication Change My Blood Sugar Levels
This is the foundational question. Levothyroxine usually raises insulin requirements modestly. Antithyroid drugs usually lower them. Knowing the direction of expected change helps you watch for patterns rather than being surprised by them.
How Should I Time This Medication Relative to My Diabetes Drugs
Confirm the morning routine: thyroid med, then a 30 to 60 minute wait, then breakfast and diabetes medications. Ask whether anything in your specific regimen needs more space.
How Often Should My Thyroid Levels Be Rechecked
The Endocrine Society recommends rechecking TSH about six to eight weeks after any dose change, and then every six to twelve months once stable. People with diabetes may benefit from slightly more frequent checks during the adjustment period because of the metabolic ripple effects.
What Symptoms Should I Report
Common signs that the thyroid dose needs adjustment include increased fatigue, mood shifts, palpitations, weight changes, and noticeable shifts in blood sugar patterns. The ADA Standards of Care emphasize that symptom changes in someone with both conditions should prompt evaluation of both, not just one.
Should My Diabetes Medication Doses Be Adjusted
Ask whether your diabetes drugs may need temporary or permanent changes during the thyroid adjustment period. Some endocrinologists are comfortable adjusting both at once. Others prefer to coordinate with your diabetes provider, especially if you use insulin or take multiple oral medications.
Are There Any Supplements or Foods I Should Avoid
Calcium, iron, soy products in large amounts, and high-fiber meals taken too close to levothyroxine can blunt absorption. A pharmacist can review your supplement list and flag anything that might interfere.
For more on advocating for yourself with medication-heavy regimens, our guide on blood pressure medication questions for people with diabetes covers a similar conversation framework.
Understanding Thyroid Medication Basics
Thyroid medications fall into two main categories: hormone replacement and antithyroid drugs. Knowing which group your medication belongs to helps you predict its effects.
Levothyroxine (Synthroid, Levoxyl, Tirosint, Generic)
Levothyroxine is a synthetic version of T4, the main hormone the thyroid produces. The body converts it to T3, the active form, as needed. It is used for hypothyroidism, including the kind caused by Hashimoto's thyroiditis. Doses are individualized based on TSH and symptoms, and consistency matters more than the absolute number.
Liothyronine and Combination Therapy
Some people do not feel well on T4 alone and may benefit from added T3 (liothyronine) or a combination product. The evidence on routine combination therapy is mixed, but it is an option for people whose symptoms persist despite normal TSH on levothyroxine alone.
Methimazole and Propylthiouracil (PTU)
Antithyroid drugs are used for hyperthyroidism, including Graves' disease. They block the thyroid's ability to make hormone. Methimazole is usually first-line, and PTU is preferred in the first trimester of pregnancy. Both can affect blood counts and liver function, so monitoring labs are part of the routine.
Why Dosage Stability Matters for Both Conditions
Frequent thyroid dose changes ripple into blood sugar variability. Once a dose is dialed in, sticking with the same brand or generic, taking it at the same time each day, and avoiding interactions can keep both thyroid and glucose levels predictable. Switching brands midstream is a common reason for surprise blood sugar shifts.
Hypothyroidism Treatment and Blood Sugar
Starting levothyroxine for the first time, or after a long stretch of being undertreated, often produces noticeable blood sugar changes within four to twelve weeks.
What to Expect in the First Month
In the first month, most people feel a gradual lift in energy, slightly faster digestion, and small shifts in appetite. Blood sugar changes may not be obvious yet, but a CGM often shows subtle pattern shifts. This is a good window to keep a more detailed food and glucose log so you can spot trends before they become problems.
Months Two and Three
Insulin sensitivity often shifts more noticeably in months two and three as thyroid hormone reaches a steady state. People on insulin may find basal needs go up by 5 to 15 percent. People on metformin or other oral drugs sometimes notice fasting glucose drops because the liver's morning glucose dump becomes more efficient again.
Achieving Stable Thyroid Levels
Stable thyroid levels usually mean stable blood sugar patterns. Once your TSH has been in a steady range for six months, day-to-day fluctuations from thyroid factors largely disappear. The remaining variability is from the usual suspects: meals, stress, sleep, and activity.
For deeper coverage of the long-term picture, see our guide on managing hypothyroidism and diabetes together.
From my experience: when I started levothyroxine in my twenties, my endocrinologist warned me to expect a small uptick in basal insulin within two months. That is exactly what happened. My CGM showed a slow creep upward in overnight numbers, and we adjusted my pump basal by about 10 percent. The change was not dramatic, but knowing it was coming meant I did not panic when I saw the numbers shift.
Thyroid Levels and Blood Sugar Connection
The link between thyroid levels and blood sugar is not always immediate, but the patterns become clear when you watch over weeks rather than days.
How TSH Changes Correlate with Blood Sugar
When TSH drifts up (toward hypothyroidism), insulin sensitivity usually increases short-term, and people may see more lows. When TSH drifts down (toward hyperthyroidism), insulin needs typically rise, and people may see more highs. The correlation is not perfect, but it is strong enough to use as a working hypothesis when patterns shift.
The Lag Between Dose Changes and Blood Sugar Effects
Levothyroxine has a long half-life of about a week, so it takes four to six weeks for a dose change to fully reach steady state. Blood sugar effects typically follow at a similar pace. This is why labs are repeated about six to eight weeks after a change rather than immediately.
Monitoring Strategies for the Adjustment Period
A CGM is the most useful tool during a thyroid dose change. It shows the slow drift in patterns that fingersticks miss. If you do not use a CGM, more frequent fingerstick checks (especially fasting and bedtime) provide a similar picture, just with more effort.
Keeping a simple log of TSH dates, dose changes, and any noticeable blood sugar pattern shifts gives you and your provider a useful timeline at follow-up visits.
The Importance of the TSH Blood Test
The TSH blood test is the cornerstone of thyroid medication management. It guides dose adjustments, confirms that treatment is working, and catches drift before symptoms become significant.
How TSH Testing Guides Thyroid Medication Dosing
Doctors aim to keep TSH within a target range, often 0.5 to 2.5 mIU/L for people on thyroid hormone replacement, though the exact target is individualized. If TSH drifts above the range, the dose may need to go up. If it drifts below, the dose may need to come down.
Recommended Testing Frequency
For people taking thyroid medication and managing diabetes:
- Six to eight weeks after starting or changing a dose: confirm the change is working.
- Every six to twelve months once stable: routine monitoring.
- Sooner: if symptoms or blood sugar patterns shift unexpectedly.
What to Do When TSH and Blood Sugar Change Simultaneously
If both numbers shift in the same direction, the thyroid is likely the upstream cause. If they move in opposite directions, something else is going on, such as diet changes, illness, stress, or another medication. Sharing both data sets with your provider helps them sort out which lever to pull.
For more on what your TSH number actually means in the context of diabetes, our deep dive on what a TSH blood test means walks through the ranges and the practical implications.
You can also explore our broader piece on how thyroid affects blood sugar levels for the underlying mechanisms.
A Practical Next Step
Before your next appointment, write down two or three specific questions about your thyroid medication and how it might be affecting your blood sugar. Bring a recent week of glucose data if you have it. The combination of focused questions and concrete numbers turns a routine visit into a useful conversation, and small adjustments often make a big difference in day-to-day stability.
FAQ
How does thyroid medication interact with diabetes drugs?
Thyroid hormone replacement (levothyroxine) can increase blood sugar by speeding up metabolism, which may require adjusting diabetes medication doses. Antithyroid drugs do the opposite. The timing of when you take each medication also matters, as levothyroxine should be taken on an empty stomach.
What should people with diabetes ask about thyroid medication?
Key questions include whether the medication will affect blood sugar, how to time it with diabetes drugs, how often thyroid levels should be rechecked, what symptoms to report, and whether insulin or oral medication doses need adjustment during thyroid treatment changes.
Can levothyroxine raise blood sugar?
Yes, modestly. As metabolism normalizes, glucose absorption and liver glucose output speed back up, which can raise insulin needs by 5 to 15 percent during the first few months of treatment.
How long after starting thyroid medication will my blood sugar change?
Most people notice gradual shifts over four to twelve weeks. The full effect typically settles in by month three, when thyroid hormone levels have stabilized.
Should I take my thyroid medication and insulin at the same time?
You can, as long as the levothyroxine is taken on an empty stomach with water. Most people take levothyroxine first thing in the morning, then wait 30 to 60 minutes before eating breakfast and taking other medications, including mealtime insulin.
The honest summary on thyroid medication diabetes interactions is that most are small, predictable, and manageable when you and your provider know what to expect. Bring focused questions, a week of glucose data, and an honest read of how you feel. Small dose changes during the adjustment window are normal, and a coordinated plan between your endocrinologist, primary care provider, and pharmacist keeps the rest of your routine steady.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.