TSH Blood Test: What It Means for Diabetes
Understand the TSH blood test, what its results mean for blood sugar, and why diabetes raises your risk of thyroid disease.

In this article(17)
A TSH blood test is one of the most important screening tools for people with diabetes, yet many of us do not know what the number on the lab report actually measures. Thyroid disease and diabetes overlap far more than chance would predict, and a quiet shift in thyroid function can throw off blood sugar readings, energy, weight, and sleep all at once. Catching that shift early through a routine thyroid screen can save months of frustrating glucose readings and unexplained fatigue.
This guide breaks down what TSH measures, why your endocrinologist orders it more often than the average primary care doctor, and how to read your results in the context of diabetes. We use plain language, link to the major medical sources, and keep the discussion focused on what helps you have a more useful conversation with your care team.
What Is a TSH Blood Test
TSH stands for thyroid-stimulating hormone. It is produced by the pituitary gland, a small structure at the base of the brain, and its job is to tell the thyroid gland in the front of your neck how much thyroid hormone to make. When the body senses low circulating thyroid hormone, the pituitary releases more TSH. When thyroid hormone is high, TSH drops. The relationship is inverse, which trips up a lot of people the first time they read a lab report.
A TSH blood test is a simple blood draw, usually from a vein in the arm. There is no need to fast for most TSH tests, though some labs prefer a morning draw because TSH levels naturally fluctuate through the day. Results typically come back within a day or two and are reported in milli-international units per liter, written as mIU/L.
According to the American Thyroid Association, TSH is the most sensitive screen for thyroid dysfunction in most adults. A small change in thyroid hormone causes a much larger change in TSH, which is why it is the first test ordered when a doctor suspects a thyroid problem.
What the Test Actually Measures
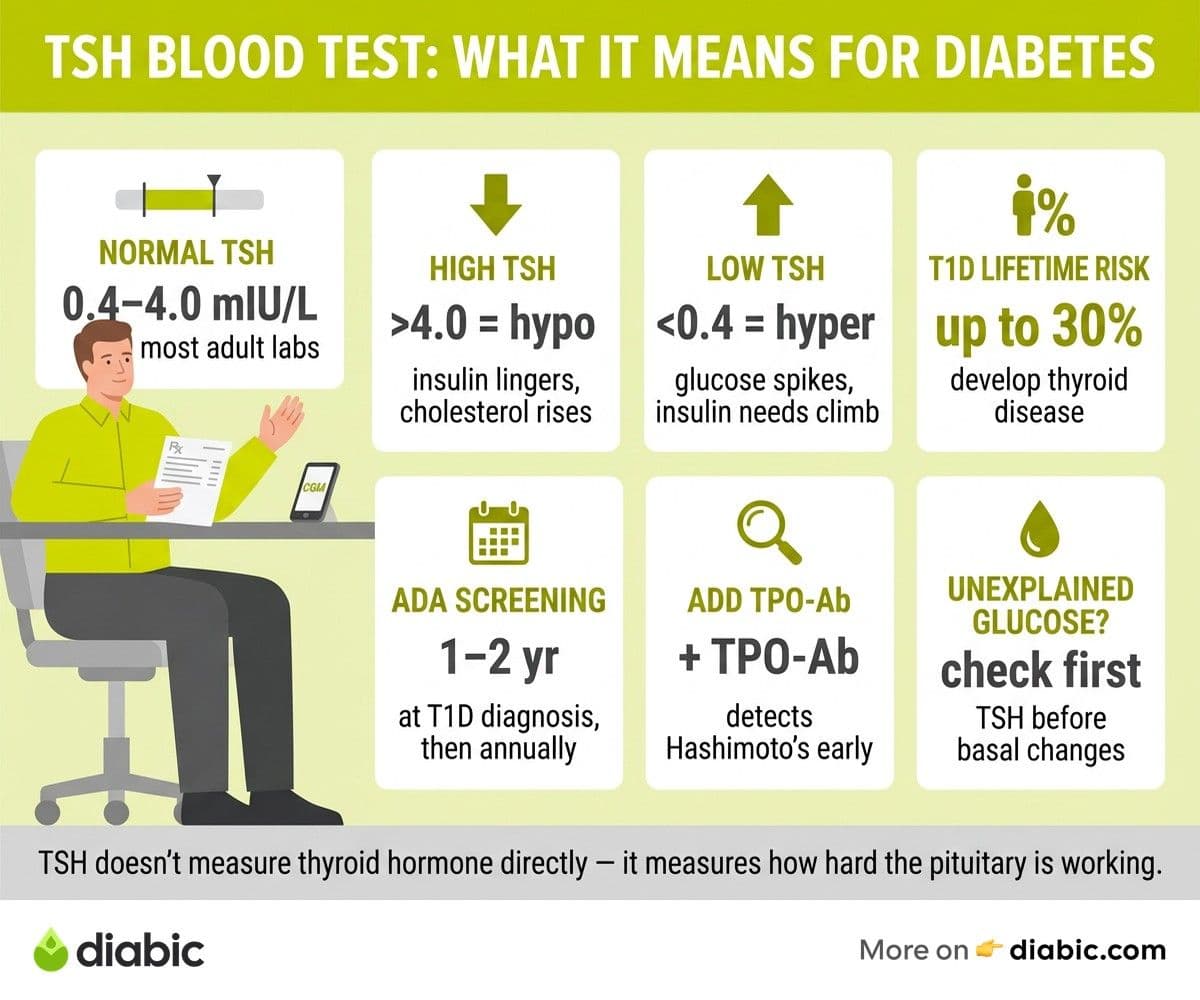
The thyroid stimulating hormone test does not measure thyroid hormone directly. It measures how hard the pituitary is working to push the thyroid into action. A high TSH suggests the thyroid is underperforming and the pituitary is shouting at it. A low TSH suggests the thyroid is overactive and the pituitary has stopped sending signals because there is already enough hormone in circulation.
This is why the TSH test is sometimes followed by a free T4 or free T3 test. Those tests measure the active hormones themselves and help confirm what the TSH is suggesting. Your doctor may order all three together if symptoms are unclear or if previous results have been borderline.
Why Should People with Diabetes Get Thyroid Screening
People with diabetes carry a higher risk of thyroid disease than the general population, and the link is strongest in Type 1 diabetes. Both conditions are autoimmune, and the immune system that attacks insulin-producing cells often goes after the thyroid as well. Hashimoto's thyroiditis, which causes hypothyroidism, and Graves' disease, which causes hyperthyroidism, both appear at higher rates in people with Type 1.
The American Diabetes Association Standards of Care recommend thyroid function screening at diagnosis of Type 1 diabetes and periodically thereafter, especially when symptoms suggest a problem or when blood sugar patterns shift without clear cause. People with Type 2 diabetes also have an elevated risk, particularly women over 50 and anyone with a family history of thyroid disease. A 2019 review in the NIDDK library noted that thyroid disorders affect up to 30 percent of people with Type 1 diabetes during their lifetime.
The connection runs in both directions. Untreated hypothyroidism can mimic diabetic symptoms like fatigue, weight gain, and brain fog. Untreated hyperthyroidism can produce unexplained highs, weight loss, and a faster heart rate that may be mistaken for stress or insulin sensitivity changes. Either condition can quietly destabilize what was once steady glucose control.
If you live with both, our piece on managing hypothyroidism and diabetes walks through how to coordinate care between your endocrinologist and primary care team without duplicating tests or missing signals.
What Do TSH Results Mean for Diabetes
TSH results are best understood as a range rather than a single magic number. Reference ranges vary slightly by lab, but most adult labs use roughly 0.4 to 4.0 mIU/L as normal. The Mayo Clinic notes that "normal" can shift with age, pregnancy status, and medications, so results should always be interpreted alongside symptoms and history.
Normal TSH Range
A TSH between roughly 0.4 and 4.0 mIU/L generally means the pituitary and thyroid are working together as expected. For most people with diabetes, a normal TSH is one less variable to worry about. That said, what counts as normal for you may not be the textbook range. Some endocrinologists treat TSH above 2.5 in patients with autoimmune markers or symptoms, especially in pregnancy, while others wait until results clearly cross the standard threshold.
High TSH and Hypothyroidism
A TSH above the lab's upper limit, often 4.0 to 4.5 mIU/L, suggests hypothyroidism. The thyroid is making too little hormone, the pituitary is pushing harder, and the body slows down. Symptoms include fatigue, cold intolerance, dry skin, constipation, weight gain, and sluggish thinking. Hypothyroidism can also raise LDL cholesterol and shift A1C trends in ways that make diabetes harder to read.
For people with diabetes, untreated hypothyroidism can blunt insulin sensitivity in some ways and increase the risk of hypoglycemia in others, depending on individual physiology. Treatment with levothyroxine, a synthetic thyroid hormone, often stabilizes both energy and glucose patterns within a few months. Always confirm dose changes with your prescriber rather than self-adjusting.
Low TSH and Hyperthyroidism
A TSH below the lab's lower limit, often 0.3 to 0.4 mIU/L, suggests hyperthyroidism. The thyroid is making too much hormone, the pituitary has scaled back its signal, and the body speeds up. Symptoms include rapid heart rate, weight loss, anxiety, heat intolerance, hand tremor, and trouble sleeping. In Type 1 diabetes, Graves' disease is the most common cause, and our piece on recognizing symptoms of Graves' disease with diabetes covers what to watch for.
Hyperthyroidism often raises blood sugar and increases insulin requirements. People who pump may need basal rate adjustments, and those on multiple daily injections may notice their usual carb ratios stop working. Treatment may involve antithyroid medications, radioactive iodine, or surgery, all of which require coordinated care with an endocrinologist.
From my experience: After 14 years of living with Type 1 diabetes, I have watched my TSH move into the upper end of normal more than once during periods of stress and poor sleep. The first time my numbers crept up, my time in range dropped before any classic thyroid symptom appeared. The lesson I keep relearning is to treat unexplained shifts in glucose patterns as a reason to ask my care team for a thyroid panel, not just to chase basal rate changes.
Understanding the TSH Test in Context
A single TSH result rarely tells the whole story. The thyroid system responds to stress, illness, certain medications, and time of day. A TSH drawn during the flu may look different from one drawn in your normal baseline state. Repeat testing in four to six weeks is often more useful than reacting to a single borderline value.
When TSH Alone Is Not Enough
For people with diabetes, doctors often pair the TSH test with free T4, free T3, and thyroid antibody tests like TPO antibodies. The antibody panel is especially useful in Type 1 because a positive result can predict future thyroid disease even when TSH is still in the normal range. The Endocrine Society publishes detailed guidance on when to add these supplemental tests.
Pregnancy changes everything. Thyroid demands rise in early pregnancy, and the reference ranges shift. If you are pregnant or planning to be, talk to your provider about a more conservative TSH target.
Medications and Conditions That Skew Results
Several common medications affect TSH or thyroid hormone levels. Metformin, biotin supplements, glucocorticoids, lithium, and amiodarone can all influence results. So can severe illness, recent surgery, and significant weight loss. Mention every supplement and prescription to your doctor before a thyroid panel, and our thyroid medication questions piece covers the conversation in more detail.
Thyroid Stimulating Hormone Test and Blood Sugar
Thyroid hormone influences nearly every metabolic process, which is why thyroid problems and diabetes are so deeply intertwined. Hyperthyroidism speeds up gut absorption of glucose, increases hepatic glucose output, and raises insulin clearance. The result is often higher glucose readings and more insulin needed per gram of carbohydrate.
Hypothyroidism slows gluconeogenesis and reduces insulin clearance, which can sometimes lower fasting glucose but also extend the action of insulin in unpredictable ways. People with hypothyroidism on insulin therapy sometimes report more low blood sugars, especially overnight, until the thyroid is treated.
Correcting thyroid dysfunction often improves both A1C trends and time in range. It is not unusual for someone newly treated for hypothyroidism to see their basal insulin needs change within the first three months on levothyroxine. The key is coordination, not a one-size-fits-all rule.
Thyroid and Blood Sugar Management
Building thyroid monitoring into routine diabetes care is straightforward once it becomes a habit. Most people with Type 1 diabetes do well with a TSH check at least once a year, more often if symptoms suggest a problem. People with Type 2 diabetes can ask about adding TSH to their annual lab panel, especially after age 50 or with a family history of thyroid disease.
If you take levothyroxine, timing matters. Most providers recommend taking it on an empty stomach 30 to 60 minutes before food, coffee, or other medications, including some diabetes pills. Calcium and iron supplements should be separated by several hours. Consistency helps your TSH stabilize and gives your care team a clearer picture of whether the dose is right.
Coordinating between an endocrinologist and a primary care physician sometimes means making sure neither assumes the other has ordered the test. Ask which provider runs your thyroid panel and when. Our piece on how thyroid affects blood sugar levels covers the daily management side of life with both conditions.
Putting the Number in Perspective
A TSH result is data, not a verdict. It is one signal among many, and it has real value when interpreted in the context of your symptoms, your other labs, and your diabetes history. Trust the trend more than any single number, ask questions about borderline results, and treat thyroid screening as part of normal diabetes care rather than an extra task.
If your screening result shows something unexpected, do not panic. Most thyroid issues respond well to treatment, and getting the right diagnosis often makes diabetes feel more predictable again. Schedule the conversation, bring your CGM data and symptom notes, and let your care team translate the numbers into a plan.
Frequently Asked Questions
Why should people with diabetes get a TSH blood test?
People with diabetes, especially Type 1, have a significantly higher risk of thyroid disorders due to shared autoimmune mechanisms. Undetected thyroid problems can cause unexplained blood sugar fluctuations, fatigue, and weight changes that may be mistaken for diabetes management issues. Regular TSH screening, as recommended by the American Diabetes Association, catches these issues early and supports more stable glucose patterns.
What do TSH results mean for diabetes?
A high TSH suggests hypothyroidism, which can slow metabolism, alter insulin sensitivity, and shift A1C trends in confusing ways. A low TSH suggests hyperthyroidism, which can raise blood sugar and increase insulin requirements. Both scenarios usually require treatment adjustments, and correcting thyroid dysfunction often stabilizes blood sugar within a few months.
How often should people with diabetes get screened?
Most clinicians recommend thyroid screening at the time of Type 1 diabetes diagnosis and at least once a year afterward, or sooner if symptoms or unexplained glucose patterns appear. People with Type 2 diabetes can ask their provider about adding TSH to annual labs, particularly after age 50 or with a family history of thyroid disease. Talk to your doctor about a screening schedule that fits your history.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.