A1C Normal Range: What Your Results Mean
The A1C normal range tells you more than daily readings can. Learn the chart, conversion to eAG, what skews results, and how often to test.

In this article(9)
Your A1C normal range tells you a story your daily blood sugar numbers cannot. It is a single percentage that reflects your average blood glucose over the past two to three months, and knowing where you fall on the scale is one of the most important parts of your diabetes picture. Whether you are newly diagnosed, navigating prediabetes, or several years into managing diabetes, the A1C is the long-view anchor your provider keeps coming back to.
The numbers themselves are easy to memorize. The harder part is understanding what your specific result means for your situation, what factors might be making the test less accurate for you, and what you can actually do to move the number in the right direction. This guide walks through each piece in order.
What Is the A1C Normal Range
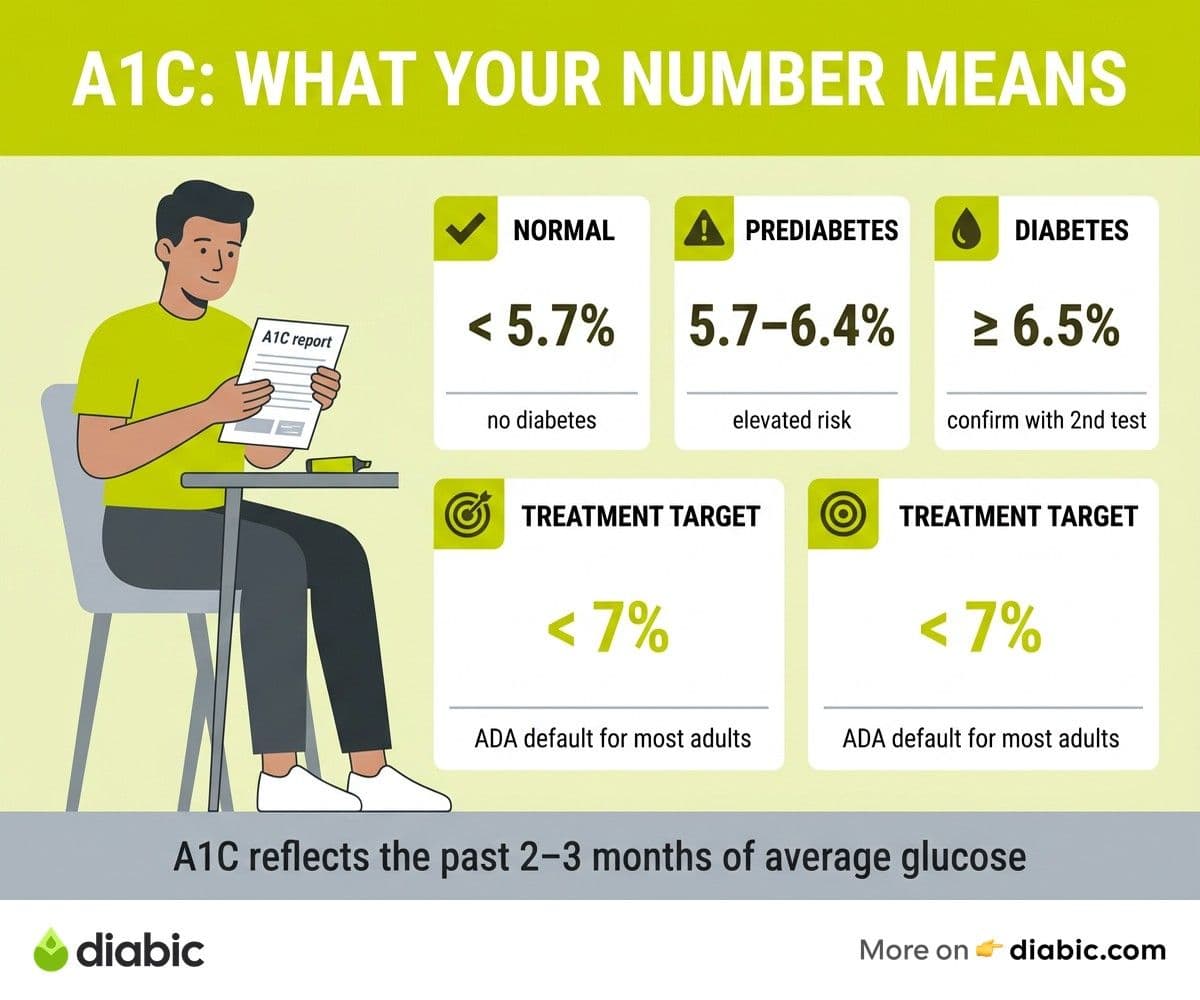
The American Diabetes Association sets the standard ranges that nearly every clinic in the United States uses. They are straightforward:
- Normal: below 5.7 percent
- Prediabetes: 5.7 percent to 6.4 percent
- Diabetes: 6.5 percent or higher
For most non-pregnant adults already living with diabetes, the ADA Standards of Care recommend a treatment target of below 7 percent. That target represents a balance: low enough to substantially reduce the risk of long-term complications, but not so low that hypoglycemia becomes a frequent problem.
Treatment targets are not one-size-fits-all. Your provider may set a different goal based on factors like your age, how long you have lived with diabetes, your history of severe lows, other medical conditions, and life expectancy. Older adults with multiple chronic conditions may have a target of 7.5 to 8 percent because the risks of intensive glucose lowering can outweigh the benefits in that group. Pregnant individuals or those planning pregnancy often have tighter targets in the 6 to 6.5 percent range, set in close collaboration with their endocrine and obstetric teams.
A few important nuances. First, the diagnostic ranges (normal, prediabetes, diabetes) and treatment targets are different things. Once you have a diabetes diagnosis, the conversation moves from "what category am I in" to "what is the safest, most effective target for me." Second, the diagnosis itself usually requires confirmation with a second test rather than a single elevated A1C. The ADA recommends a repeat A1C, a fasting plasma glucose, or an oral glucose tolerance test for confirmation in most cases.
The A1C standardization that makes these ranges meaningful comes from the National Glycohemoglobin Standardization Program (NGSP). NGSP-certified labs report results that are comparable across the country, which is why a 6.7 percent in one clinic means roughly the same thing as a 6.7 percent in another.
What Does Your A1C Number Mean
A1C measures the percentage of your hemoglobin (the oxygen-carrying protein in red blood cells) that has glucose attached to it. When blood glucose is high over time, more of your hemoglobin gets coated with glucose. When blood glucose is well managed, less of it does. Because red blood cells live about 120 days, the A1C reflects roughly the past two to three months of average glucose, with more weight on the most recent month. For a deeper look at the underlying biology, our guide on glycohemoglobin A1C explained walks through the science.
The most useful translation for daily life is the conversion from A1C percentage to estimated average glucose (eAG), which is the number you would see on your meter. The ADA eAG calculator uses this formula:
The conversion table is a reality check. Many people are surprised the first time they see it. An A1C of 8 percent means an average blood glucose of 183 mg/dL across all hours of all days. If your fingersticks show readings in the 130s most of the time, an A1C of 8 is telling you that something is happening when you are not testing, often overnight or in the hours after meals.
Why two to three months and not, say, six? Red blood cells are continuously made and replaced. Newer cells have had less time to accumulate glucose attachment, while older cells have been exposed for longer. The A1C is essentially a weighted average of all these cells, which is why the most recent four to six weeks have a stronger influence on the result than older time periods. A change in your routine made a month ago will show up partially in your next A1C and more fully in the one after.
Factors That Affect Your A1C Results
A1C is reliable for most people most of the time, but several conditions can push the result up or down without any change in actual glucose levels. Knowing these is part of interpreting your number honestly.
Anemias and hemoglobin variants. Iron-deficiency anemia and vitamin B12 deficiency can falsely raise A1C because red blood cells live longer and accumulate more glucose attachment. Hemolytic anemia, recent blood loss, and recent transfusions can falsely lower it because new cells replace older ones faster than usual. Hemoglobin variants like HbS (sickle cell trait), HbC, and HbE can interfere with some A1C assays, though most modern assays handle the common variants well.
Kidney and liver disease. Severe kidney disease can produce artifacts that raise A1C above what glucose levels alone would predict. Advanced liver disease can affect both glucose levels and A1C reliability. In both cases, your provider may rely more on alternative measures like fructosamine or CGM data.
Pregnancy. Red blood cell turnover increases during pregnancy, which tends to lower A1C. This is one reason pregnancy targets are set lower and why providers also use other tests during pregnancy to monitor glucose patterns more precisely.
Race and ethnicity. Research has found that average A1C values can differ slightly across racial and ethnic groups at the same average glucose level. A study by Herman and Cohen published in JCEM (2012) reported that Black adults averaged about 0.4 percentage points higher than white adults at matched glucose levels. The clinical takeaway is not that the test is invalid, but that providers should consider context, especially around borderline results.
When A1C does not match your daily readings. This is one of the most useful clinical signals. If your meter or CGM consistently shows readings that would suggest an A1C of 6.5, but your lab A1C comes back at 8, one of the factors above may be at play. The reverse can happen too. Beyond medical conditions, glucose variability plays a role: high spikes followed by lows can average to a number that hides the volatility. The fix is not to panic about the lab number. It is to ask your provider what alternative measures might give a clearer picture for your situation.
From my experience: My first endocrinologist taught me to look at A1C as one of three numbers, not the only one. The other two were time in range and average glucose from my CGM. After 14 years of this, I still get an A1C every three months, but it carries about a third of the weight in our conversations. The trend over time and the patterns in my CGM data carry the rest. That balance has been more useful than any single number ever was on its own.
How Often Should You Get an A1C Test
ADA guidance on testing frequency is clear, with some flexibility built in:
- At least twice a year for people with stable diabetes management who are meeting their treatment target
- Every three months for people whose treatment has recently changed or who are not at target
- More often during pregnancy, after major treatment changes, or in any situation where close monitoring is clinically indicated
Newly diagnosed people often have A1C checked more frequently in the first year as treatment is dialed in. After that, twice a year is the floor for most people, with quarterly testing being common. The CDC overview of A1C testing supports this approach as standard.
At-home A1C test kits exist and have become more accurate in recent years, but they are not a replacement for the lab test in most cases. They can be useful for an interim check between provider visits, and some are NGSP-certified. The accuracy is generally close to the lab but not identical, so results from at-home kits should be confirmed with a lab test before any major treatment decisions. They are also not a substitute for daily monitoring with a meter or CGM, which gives you the actionable data you need for day-to-day decisions. If you are looking at home testing more broadly, our roundup of the best blood glucose meters covers the most reliable options.
A1C testing requires no fasting and no special prep. It is a simple blood draw, usually from a vein in your arm, though some clinics use fingerstick samples for in-office testing. You can eat normally before the test, take your medications as usual, and continue your routine. Hydration and a normal night of sleep are the only mild preparations worth thinking about, mostly to make the blood draw itself easier.
How to Improve Your A1C
Improving your A1C is rarely about one big change. It is usually about several smaller adjustments to the patterns that quietly shape your average glucose. Here are the levers that move it most reliably:
Reduce post-meal spikes. Post-meal glucose excursions often contribute more to A1C than fasting numbers do, especially for people whose fasting readings are already in target range. Carb awareness, meal pacing, and pre-bolusing insulin (for those who use it) are the most effective tools. Even modest reductions in peak post-meal glucose can lower A1C meaningfully over a few months.
Medication adherence and timing. Taking medications at consistent times, eating at consistent times relative to those medications, and not skipping doses on busy days all add up. If your medication regimen feels hard to stick with, that is a conversation worth having with your provider rather than a personal failure to push through. There is almost always a simpler regimen that fits better.
Exercise. Regular physical activity improves insulin sensitivity, which lowers both fasting and post-meal glucose. The ADA recommends at least 150 minutes per week of moderate-intensity aerobic activity, plus two to three sessions of resistance training. The effect on A1C from consistent exercise is well documented in the DCCT/EDIC and follow-up trials, with reductions of 0.5 to 1 percentage point common when activity becomes a regular habit.
CGM-guided adjustments. If you wear a CGM, the data lets you see exactly where your glucose runs out of range and for how long. That visibility is what makes precise adjustments possible. Looking at time in range data alongside your A1C trend often reveals which patterns are pulling your average up.
Realistic improvement goals. A common mistake is aiming for a one or two percentage point drop in three months. That pace is rare, often requires aggressive treatment intensification, and tends to come with more hypoglycemia. A reasonable target for most people is a 0.3 to 0.5 percentage point drop over three to six months, sustained, before pushing further. Progress that holds beats progress that bounces back.
A note on when to call your provider: if your A1C has trended up two or more visits in a row, if it is more than 0.5 above your target, or if you are experiencing frequent lows, those are clear reasons to schedule a conversation rather than wait for the next routine appointment.
FAQ
What is a normal A1C level for adults?
A normal A1C for adults without diabetes is below 5.7 percent. Results between 5.7 and 6.4 percent indicate prediabetes, and 6.5 percent or higher indicates diabetes (typically confirmed with a second test). For people already living with diabetes, the typical treatment target is below 7 percent, though the right target depends on your individual situation and your provider's recommendation.
What A1C level indicates diabetes?
An A1C of 6.5 percent or higher meets the threshold for a diabetes diagnosis. The ADA generally recommends confirming this with a second test (a repeat A1C, a fasting plasma glucose, or an oral glucose tolerance test) before making the diagnosis official, unless symptoms are clearly present or other criteria are unambiguously met.
How often should you get an A1C test?
The ADA recommends at least twice a year for people with stable diabetes management who are at their target, and every three months for anyone whose treatment has changed recently or who is not at target. Newly diagnosed people, those in pregnancy, and those undergoing major treatment changes may need more frequent testing.
Knowing your A1C normal range and where your number sits is the start, not the end, of the conversation. Pair it with daily monitoring, talk to your doctor about what target makes sense for you, and treat the number as a guide rather than a grade. Small consistent adjustments to your routine show up in the A1C three months later, which is one of the more reassuring patterns in diabetes care.
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Devices & Technology
View all
Using a Continuous Glucose Monitor for Hypoglycemia
A continuous glucose monitor for hypoglycemia can catch lows before symptoms hit. Learn how alerts, trends, and CGM data help prevent severe episodes.

Best Continuous Glucose Monitors for Type 2 Diabetes in 2026
Compare the best continuous glucose monitor for type 2 diabetes options, including Stelo, FreeStyle Libre 3, and Dexcom G7, with pricing and accuracy.

Best Blood Glucose Meters for Home Testing in 2026
Compare the best blood glucose meter options for home testing in 2026, including accuracy ratings, strip costs, and features that matter day to day.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.