Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

In this article(23)
You sit down with a cup of coffee and your tongue feels scalded, even though the coffee is barely warm. The sensation lingers, sometimes worse by evening, sometimes vanishing during meals only to creep back later. If this is familiar, you may be experiencing burning mouth syndrome, and the burning mouth syndrome diabetes connection is one many people never get a clear answer about until they raise it themselves.
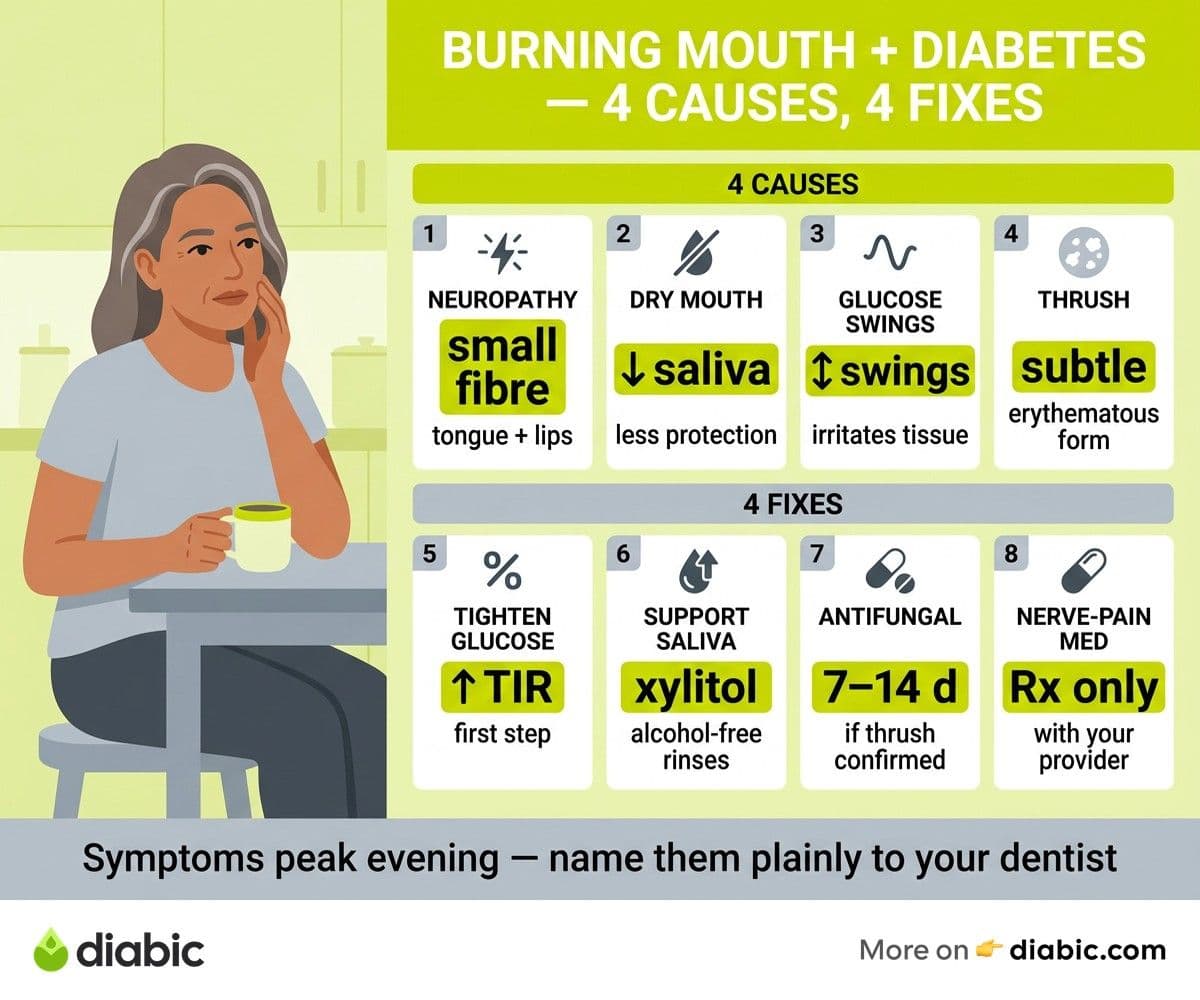
Burning mouth syndrome (BMS) is a chronic condition where the mouth feels burning, scalding, tingling, or numb without an obvious physical cause. For people with diabetes, the symptoms often trace back to a mix of neuropathy affecting the nerves in the mouth, dry mouth, fungal overgrowth, or fluctuating blood sugar irritating sensitive oral tissues. None of those causes is dramatic on its own, but layered together they can produce daily discomfort that wears people down.
This guide walks through what is happening in the mouth, how to tell BMS apart from related conditions, and what treatment options have evidence behind them. Most people see real relief once the underlying contributors are identified and addressed.
What Causes Burning Mouth Syndrome Diabetes Patients Often Notice
Burning mouth syndrome is usually classified as either primary, where no underlying medical cause is found, or secondary, where a specific condition explains the symptoms. The NIDCR's burning mouth overview notes that secondary BMS often traces to nerve damage, dry mouth, fungal infections, or nutritional deficiencies. In people with diabetes, the picture leans secondary, meaning the burning sensation often has identifiable contributors.
Diabetic neuropathy in oral nerves
The most studied link is small fiber neuropathy. Diabetes can damage the small unmyelinated nerve fibers that carry sensations like temperature and pain. When those fibers are affected in the tongue and oral mucosa, the result can be burning, tingling, or altered sensation. Research published in journals such as Oral Diseases has documented higher rates of BMS in people with diabetes, particularly those with longer disease duration or evidence of peripheral neuropathy elsewhere.
Chronic dry mouth
Dry mouth, or xerostomia, is common in diabetes for several reasons: high blood sugar, medications, and changes in salivary gland function. Saliva normally protects the oral tissues with moisture and antimicrobial proteins. When it is reduced, the tongue and cheek tissues become more vulnerable to mechanical irritation and to subtle nerve signaling that registers as burning. Our piece on dry mouth causes and remedies with diabetes covers this in more detail.
Blood sugar fluctuations
Periods of high glucose can change the composition of saliva and the local environment of the mouth, while episodes of low glucose can heighten nerve sensitivity. People who experience wide swings sometimes report that burning sensations track loosely with their CGM patterns. The connection is not always tidy, but worth paying attention to.
Fungal infections
Candida overgrowth, particularly subtle cases without obvious white patches, can present primarily as a burning sensation. This is sometimes called erythematous candidiasis. Because diabetes raises the risk of oral candidiasis, this is one of the first things a dentist will rule out.
Is Burning Mouth Syndrome a Sign of Diabetic Neuropathy
It can be, especially if you have been living with diabetes for several years. The NIDDK's overview of diabetic neuropathy describes several types, including peripheral neuropathy that classically affects the feet and hands and autonomic neuropathy that affects internal organs. Less commonly discussed is small fiber neuropathy, which can affect the small sensory nerves in the mouth, the skin, and elsewhere.
Burning mouth as a presentation of small fiber neuropathy tends to share features with neuropathy at other sites:
- Symptoms that are persistent rather than coming and going randomly
- A burning, tingling, or pins-and-needles quality
- A pattern of slow onset over weeks or months
- Worsening through the day, often peaking in the evening
If you have known neuropathy in your feet or hands and develop oral burning, the connection is more likely. Even without prior neuropathy, persistent oral burning is worth flagging because it can sometimes be one of the earlier signs of small fiber involvement. Our piece on recognizing diabetic peripheral neuropathy covers what to watch for elsewhere in the body.
A definitive diagnosis of small fiber neuropathy can require specialized testing such as a skin biopsy, but a thoughtful clinical exam by your provider often points the way without that step.
Symptoms of Burning Mouth Syndrome
Burning mouth syndrome diabetes presentations have a few hallmarks that help distinguish them from other oral problems. The most common is a burning or scalding sensation on the tongue, especially the tip and sides. Some people describe it as the feeling after sipping coffee that is too hot, except it does not go away.
Other reported symptoms include:
- Tingling or numbness in the tongue, lips, or roof of the mouth
- Altered taste, sometimes a metallic or bitter flavor that lingers
- Dryness that persists even with frequent water sips
- Symptoms that worsen as the day progresses
- Relief during meals, oddly enough, with the burning returning afterward
The symptoms often appear together rather than singly. Many people also notice that stress, fatigue, and dehydration intensify the discomfort, while distraction during work or conversation can dull it.
How BMS differs from other conditions
Oral thrush usually has visible white patches that wipe off, leaving red tissue underneath. Burning mouth syndrome typically has no visible changes on exam. Geographic tongue presents with patches that change shape over time and can sometimes burn, but it has a distinctive map-like appearance. Acid reflux can irritate the throat and back of the mouth, often with a sour taste. Vitamin deficiencies, including B12, folate, iron, and zinc, can also produce burning sensations and are commonly checked as part of a workup.
The American Dental Association summarizes the diagnostic process as essentially a process of ruling out identifiable causes and treating any that show up.
The Role of Dry Mouth in Burning Mouth Syndrome
Dry mouth and burning sensations often travel together. In a healthy mouth, saliva forms a thin protective film over the tissues and contains buffers, enzymes, and antimicrobial proteins. When that film thins out, the tongue rubs against teeth and palate with less cushion, the tissues become more sensitive, and small irritations register more loudly.
For people with diabetes, the cycle can become self-reinforcing. High blood sugar contributes to dry mouth, dry mouth contributes to local irritation, irritation increases the perception of burning, and any subtle nerve sensitivity gets amplified by the lack of moisture. Treating the dry mouth piece often quiets the burning even when neuropathy is in the mix.
Practical strategies that may help:
- Sip water steadily through the day rather than gulping it occasionally
- Chew sugar-free gum with xylitol to stimulate saliva
- Use over-the-counter saliva substitutes or moisturizing oral gels
- Avoid alcohol-based mouthwashes, which dry tissues further
- Limit acidic and spicy foods if they trigger flares
If dry mouth is severe, your dentist may recommend prescription products like pilocarpine, which stimulates saliva production. This is a conversation to have with both your dentist and your diabetes care team, since some of those medications interact with other parts of your regimen.
Oral Thrush and Its Connection to Burning Mouth
Some cases of burning mouth in people with diabetes turn out to be oral thrush in a less obvious form. Erythematous, or atrophic, candidiasis presents primarily as red, sore tissue rather than the cottage-cheese white patches most people associate with thrush. The dominant symptom is often burning, particularly on the tongue and palate.
Because high blood sugar promotes Candida overgrowth in the mouth, this form of thrush is more common in diabetes than in the general population. It can persist quietly for weeks or months while the person assumes they have a chronic burning sensation from another cause. A dentist can often identify it on exam, sometimes with a swab to confirm.
If a fungal cause is found, treatment with antifungal medication usually clears the burning along with the infection. This is one reason it is worth getting a thorough oral exam early in the workup rather than assuming the symptoms have a more complex source. Our piece on oral thrush and diabetes treatment walks through what those medications look like.
From my experience: After fourteen years with type 1 diabetes, I have learned to be specific when I describe symptoms to my care team. When my tongue felt off for several weeks, I almost dismissed it. Naming it as a burning sensation, mentioning my CGM patterns, and asking my dentist to actually look at the tissue led to a much faster answer than vague descriptions of feeling "weird." Specificity helps your team help you.
Treatment and Relief Options
Treatment for burning mouth syndrome diabetes cases is often layered. Addressing each contributor produces better results than chasing the burning sensation alone.
Blood sugar management as a foundation
If glucose has been running high or swinging widely, working with your diabetes team to tighten time in range often takes the edge off oral symptoms over weeks to months. This is usually the first step, both because it helps directly and because it makes the other treatments more effective.
Saliva support and rinses
Saliva substitutes, moisturizing oral gels, and prescription saliva stimulants can address the dry mouth contribution. Some people find a baking soda and water rinse soothing during flares. Avoid commercial mouthwashes with alcohol, sodium lauryl sulfate, or strong flavorings, since these can irritate sensitized tissues.
Treating fungal infection
If thrush is contributing, an antifungal medication course usually shortens recovery considerably. Persistent or recurrent cases warrant a closer look at glucose patterns and any contributing factors like inhaler use.
Nerve pain medications
For confirmed neuropathy contributing to BMS, providers sometimes prescribe medications that calm overactive sensory nerves. Options that have been studied in BMS include clonazepam (sometimes used as a topical lozenge), low-dose tricyclic antidepressants, and gabapentin or pregabalin. These are decisions to make with your provider, particularly because some interact with diabetes medications and others can affect blood sugar.
Lifestyle adjustments
Stress reduction, consistent sleep, and avoiding tobacco and excess alcohol all support both diabetes and oral nerve health. Some people find that cutting cinnamon-flavored toothpastes, mint, or acidic foods reduces flares.
When to see a dentist vs an endocrinologist
Start with your dentist for a thorough oral exam to rule out thrush, dental issues, and dry mouth contributors. If neuropathy seems likely or your blood sugar has been difficult to manage, loop in your endocrinologist or primary care provider. Some larger centers have oral medicine specialists who focus specifically on conditions like BMS, which can be a useful referral for stubborn cases.
FAQ
What causes burning mouth syndrome with diabetes?
The most common contributors are diabetic neuropathy affecting the small sensory nerves in the mouth, chronic dry mouth, fungal overgrowth, and blood sugar fluctuations that irritate oral tissues. Most cases involve more than one factor at the same time. Talk to your doctor about evaluating each one.
Is burning mouth syndrome a sign of diabetic neuropathy?
It can be. Burning mouth is sometimes an early manifestation of small fiber neuropathy, which affects the same kind of nerves involved in peripheral neuropathy elsewhere. Persistent oral burning, especially alongside known neuropathy in the feet or hands, is worth raising with your healthcare provider.
Can burning mouth syndrome go away on its own?
Some primary cases improve over time without specific treatment, but cases tied to clear contributors like dry mouth or thrush usually need targeted treatment. Improving blood sugar management often helps even when neuropathy is part of the picture.
Does burning mouth syndrome mean my diabetes is poorly managed?
Not necessarily. People with well-managed diabetes can develop BMS too, particularly after many years with the condition. That said, persistent or worsening symptoms are a reasonable trigger for a closer look at your A1C and CGM patterns.
How long does burning mouth syndrome last?
It varies widely. Cases tied to thrush or dry mouth often resolve within weeks of treatment. Cases tied to neuropathy can be longer-running, with symptoms waxing and waning. A clear treatment plan tends to shorten the timeline meaningfully.
If your mouth has been burning for more than a few weeks, that is enough reason to talk with your dentist and bring it up at your next diabetes visit. The burning mouth syndrome diabetes overlap is more common, and more treatable, than most people realize, and naming the symptom plainly to your care team usually moves things forward faster than waiting it out.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.

Diabetes and Tooth Decay: The Real Connection
Diabetes tooth decay is more than a sugar issue. Learn the real biological connection and how to prevent cavities when blood sugar runs high.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.