Recognizing Diabetic Peripheral Neuropathy Early
Learn the early signs of diabetic peripheral neuropathy, how it is diagnosed, and what steps may help slow its progression with diabetes.

In this article(11)
Diabetic peripheral neuropathy affects up to half of people with diabetes over time, but its earliest signs are often the easiest to miss. A faint tingle in your toes at night. A sock that suddenly feels bunched even though it is not. A small cut on your foot that you only notice when you take off your shoe. These small clues can show up years before nerve damage becomes obvious.
Catching this nerve damage early matters because it changes what you can do about it. While research suggests that established nerve damage is difficult to reverse, slowing or stopping its progression is often achievable with the right combination of blood sugar management, foot care, and treatment. The earlier you act, the more nerve function you protect.
This guide covers what the condition involves, the early symptoms to watch for, how it is diagnosed, and what taking action looks like after a diagnosis. We will also touch on the other types of diabetic neuropathy and why screening every year matters even if you feel fine.
What Is Diabetic Peripheral Neuropathy
It is nerve damage caused by long-term high blood sugar, and it most often affects the feet, legs, hands, and arms. It is the most common form of diabetic neuropathy and one of the most common diabetes complications overall. According to the CDC, about half of all people with diabetes will develop some form of nerve damage during their lifetime.
The damage starts at the smallest blood vessels (the vasa nervorum) that supply oxygen and nutrients to peripheral nerves. Chronic high glucose damages the lining of these vessels, reducing blood flow to nerve fibers. Over time, the nerves themselves begin to degenerate, starting with the longest nerves in the body, which is why the toes and feet are usually affected first.
The risk factors are well understood. Long duration of diabetes, persistently high A1C, smoking, high blood pressure, high cholesterol, alcohol use, and obesity all increase the chance of developing neuropathy. Vitamin deficiencies (especially B12) and other underlying conditions can compound the problem. Information from the NIDDK confirms that improving blood sugar management is the single most effective strategy for prevention.
Both type 1 and type 2 diabetes carry the risk, though the timing tends to differ. People with type 1 typically develop neuropathy after many years of disease, while people with type 2 sometimes show signs at diagnosis because they may have had elevated blood sugar for years before being diagnosed.
Early Diabetic Neuropathy Symptoms to Watch For
The earliest diabetic neuropathy symptoms are subtle and easy to dismiss. They usually start in the toes and gradually move upward in a "stocking and glove" pattern, eventually reaching the lower legs and sometimes the hands.
Tingling, often described as "pins and needles," is one of the most common first signs. It may come and go, especially at night, and many people initially think they slept on their foot wrong or that their shoes are too tight. A sensation of walking on cotton balls or gravel that is not actually there is another classic early symptom.
Numbness can develop at the same time as tingling or follow it. The numbness usually starts at the very tip of the toes and slowly extends. You may notice that water in the bath does not feel as warm to your feet as it does to your hands, or that you do not feel the texture of carpet versus tile the way you used to.
Pain is the symptom that often pushes people to seek help. It can show up as burning, sharp, stabbing, or electric-shock sensations, and it tends to be worse at night. Some people report that the weight of bedsheets becomes uncomfortable, a phenomenon called allodynia where harmless touch feels painful. The Mayo Clinic describes this as one of the more distressing aspects of peripheral neuropathy.
Other early signs to mention to your provider include muscle weakness in the feet or ankles (especially trouble lifting the foot, called foot drop), changes in the way you walk, increased clumsiness, and loss of reflexes during a routine exam. For visual context, our guide on diabetic neuropathy in feet with pictures shows what skin and structural changes can look like over time.
Types of Diabetic Neuropathy Beyond Peripheral
Peripheral neuropathy gets the most attention, but it is not the only type. Knowing the others helps you recognize symptoms that might otherwise seem unrelated to your diabetes.
Autonomic neuropathy affects the nerves that control automatic body functions like digestion, heart rate, blood pressure, sweating, and bladder function. Symptoms can include feeling full quickly after a few bites (gastroparesis), constipation or diarrhea, dizziness when standing, frequent urinary tract infections, and unexplained sweating changes. Autonomic neuropathy is also associated with hypoglycemia unawareness, where you stop feeling the warning signs of low blood sugar.
Proximal neuropathy, sometimes called diabetic amyotrophy, affects nerves in the thighs, hips, buttocks, or legs, usually on one side of the body. It often shows up as sudden, severe pain followed by weakness in the affected muscles, and it is more common in older adults with type 2 diabetes.
Focal neuropathy (also called mononeuropathy) involves damage to a single nerve, most often in the head, torso, or leg. It can cause double vision, paralysis on one side of the face (similar to Bell's palsy), or shooting pain in specific areas. Most cases of focal neuropathy improve on their own over weeks to months.
Eye-related diabetic neuropathy is one specific form worth understanding because it can affect vision and the muscles that move the eyes. Like other focal neuropathies, it often resolves over time, but it warrants a prompt evaluation.
How Diabetic Peripheral Neuropathy Is Diagnosed
A clinical exam is the foundation of diagnosis, and most of it can happen in your primary care or endocrinology office. The American Diabetes Association Standards of Care recommend that all people with type 2 diabetes be screened at diagnosis and at least annually thereafter. People with type 1 diabetes should be screened starting five years after diagnosis and annually after that.
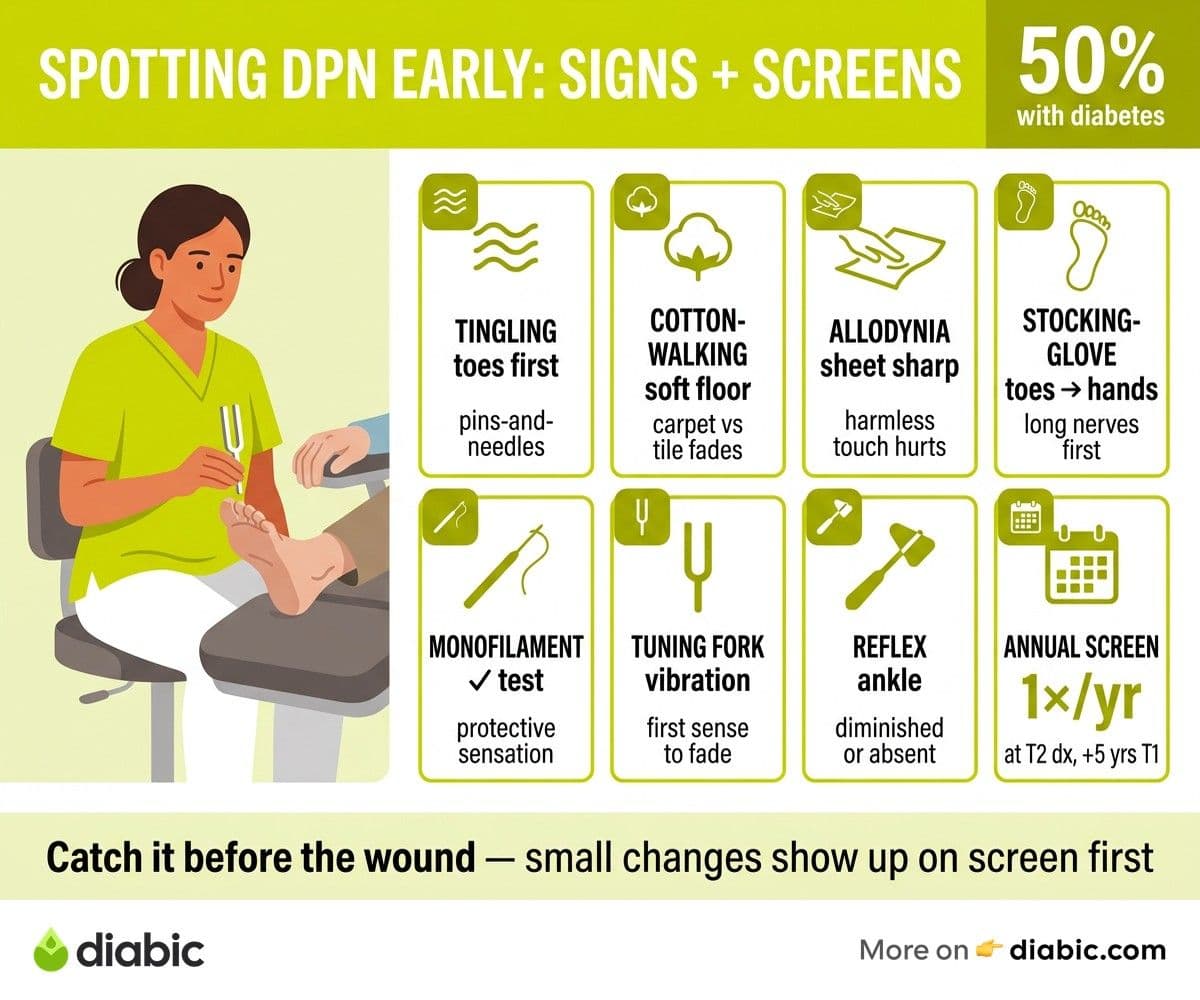
The screening exam usually includes several quick tests. A monofilament test uses a thin nylon fiber pressed against various points on the bottom of the foot to check for loss of protective sensation. A tuning fork or vibration testing device assesses how well your nerves detect vibration, which is one of the first sensations to fade. Reflex testing at the ankle, pinprick testing, and temperature sensation rounds out the basic exam.
If symptoms or exam findings suggest neuropathy, your provider may order more detailed tests. Nerve conduction studies measure how quickly electrical signals travel through your nerves, while electromyography (EMG) records the electrical activity of muscles. These tests are usually performed by a neurologist and can confirm the diagnosis as well as rule out other causes.
Blood tests are also standard at this stage. Vitamin B12 deficiency, thyroid disorders, kidney disease, and several other conditions can cause symptoms that look like diabetic neuropathy, and they need to be ruled out or addressed. A complete picture matters, because the treatment plan changes if there are multiple contributors.
The annual diabetic foot exam is more than a routine check. It is a chance to catch nerve damage before it leads to ulcers or injuries, and it is one of the most evidence-backed screening tools in diabetes care. Establishing a diabetic foot care routine is the practical complement to the annual exam.
What Happens If Neuropathy Is Not Caught Early
The progression of untreated peripheral neuropathy is what makes early detection so valuable. As nerve damage advances, sensation continues to fade, and the protective signals that keep feet safe disappear.
Loss of sensation is the gateway to many of the most serious foot complications. A small blister from new shoes, a pebble in a sock, or a minor cut can go unnoticed for hours or days. Without the pain signal that would normally make you stop and address the problem, what starts as a tiny injury can become a deep wound or infection.
Foot ulcers are the most common serious complication, and they are responsible for the majority of diabetes-related hospitalizations and amputations. Once an ulcer develops, it can be slow to heal, especially if circulation is also compromised. The good news is that ulcers are largely preventable when neuropathy is caught early and managed with daily inspection, proper footwear, and prompt attention to any small injury.
Balance and coordination are also affected by progressive neuropathy. The nerves in your feet provide constant information to your brain about your body's position in space (proprioception). When that signal weakens, the risk of falls increases, particularly at night or on uneven surfaces.
Pain that started as occasional tingling can intensify into chronic, burning, or stabbing pain that interferes with sleep, work, and daily life. Treatment options for established neuropathic pain exist, but they tend to manage symptoms rather than fully resolve them. This is why our diabetic neuropathy treatment options guide focuses on what evidence supports starting earlier rather than waiting.
From my experience: After 14 years with type 1 diabetes, my own annual foot exams have become non-negotiable, even when nothing feels off. A few years ago, my podiatrist noticed a small loss of vibration sense at my big toe before I had felt anything unusual. That early heads-up changed how I cared for my feet day to day. It also pushed me to tighten my time-in-range, which is one of the few things research consistently shows may help.
Taking Action After an Early Diagnosis
An early diagnosis is not bad news. It is the starting line for the steps that have the biggest impact on long-term outcomes.
Tightening blood sugar management is the first priority. Studies have shown that improved glycemic management can slow the progression of peripheral neuropathy, particularly in type 1 diabetes. The targets for time-in-range and A1C should be set with your care team, taking into account your hypoglycemia risk and overall health.
A treatment plan for symptoms is the second step, especially if you are experiencing pain or sleep disruption. Options include certain antidepressants, anticonvulsants, topical creams, and capsaicin patches, depending on your symptoms and medical history. Your provider can also discuss whether diabetic neuropathy can be reversed and what realistic goals look like for your specific situation.
Daily foot care becomes a foundational habit at this stage. A short routine each evening (visual inspection, gentle washing, careful drying, and moisturizing) takes only a few minutes and prevents the small problems that lead to bigger ones. Keeping your toenails trimmed straight across, wearing well-fitting shoes, and never going barefoot indoors or outdoors are also high-impact habits.
Staying physically active matters more than many people realize. Regular activity supports circulation to peripheral nerves, helps with blood sugar management, improves balance, and may reduce neuropathic pain over time. Walking, swimming, and cycling are all good options, though shoe choice and foot inspection before and after activity are especially important.
Finally, addressing other risk factors (blood pressure, cholesterol, smoking, vitamin levels) protects nerve health from multiple angles. Treating each contributor takes some effort, but the effect on long-term nerve function and overall well-being is measurable.
FAQ
What are the early signs of diabetic peripheral neuropathy?
Early signs include tingling or "pins and needles" in the toes, gradual numbness starting at the toe tips, increased sensitivity to touch (especially at night), occasional burning or sharp pain, and mild muscle weakness in the feet. Symptoms often come and go at first, which is why they are easy to overlook.
How is the condition diagnosed?
Diagnosis usually starts with a clinical foot exam that includes a monofilament test, vibration testing with a tuning fork, reflex assessment, and pinprick or temperature sensation. If results suggest neuropathy, your provider may order nerve conduction studies, EMG, and blood tests to rule out other causes like B12 deficiency or thyroid problems.
Can early treatment slow neuropathy progression?
Research suggests that improving blood sugar management can slow the progression of nerve damage, particularly in type 1 diabetes. Foot care, treating other risk factors like high blood pressure and cholesterol, staying active, and not smoking all support nerve health. Talk to your doctor about a plan tailored to your situation.
Does diabetic peripheral neuropathy go away?
Established nerve damage of this kind is generally not fully reversible. With early diagnosis and consistent management, however, progression often slows and symptoms may become more manageable. Some people experience meaningful improvement in pain or sensation as blood sugar stabilizes.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.