Diabetes and Tooth Decay: The Real Connection
Diabetes tooth decay is more than a sugar issue. Learn the real biological connection and how to prevent cavities when blood sugar runs high.

In this article(12)
You go in for a routine cleaning, expecting the usual praise about your flossing, and instead the dentist points at the X-ray and shows you two new cavities. You have not changed your brushing habits. You have not started eating candy. So how did this happen?
Diabetes tooth decay is one of the most misunderstood oral health issues, and the answer to that question rarely lives in your dietary choices alone. The connection between elevated blood sugar and cavities runs through saliva, bacterial growth, immune response, and gum health in ways that surprise most people the first time they hear them. The American Diabetes Association has long flagged tooth decay as a frequent complication, and recent research keeps adding detail to why.
This guide unpacks the real biological story. We will cover how diabetes creates conditions for decay, where dry mouth fits in, how gum disease overlaps with cavities, and the practical steps that actually protect your teeth when blood sugar runs high.
Does Diabetes Increase the Risk of Tooth Decay
Yes, and the reasons go well beyond eating habits. People with diabetes show higher rates of cavities than people without diabetes, even when their sugar intake is similar, and the difference is most pronounced when blood glucose is poorly managed. The Centers for Disease Control and Prevention lists tooth decay among the most common diabetes-related oral problems alongside gum disease.
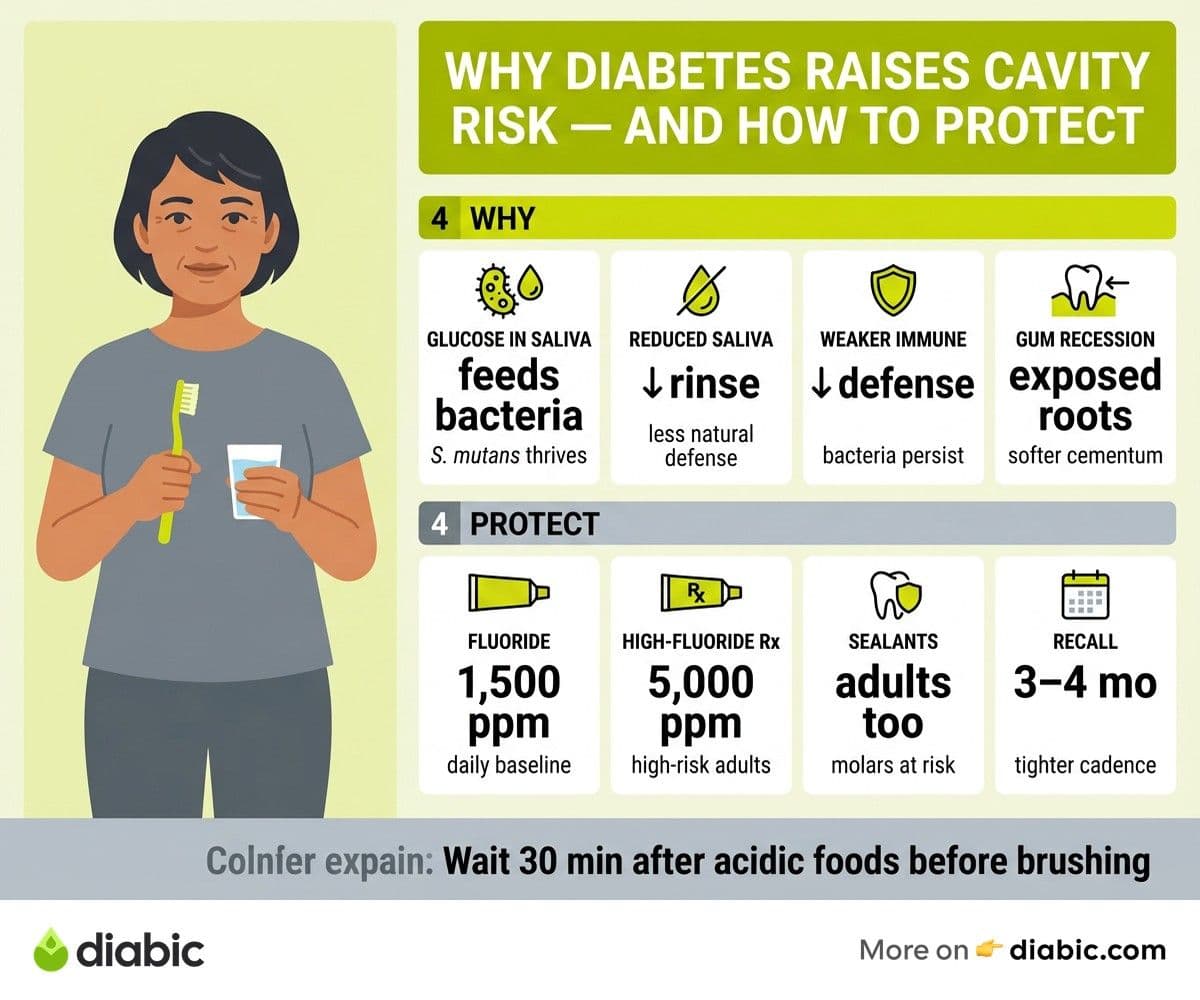
The mechanism starts in saliva. When blood glucose runs high, the glucose in your saliva rises along with it, creating a steady food supply for the bacteria that cause cavities. Streptococcus mutans, the main cavity-causing bacterium, thrives on that sugar and multiplies faster than it would in a normoglycemic mouth. More bacteria means more acid, and more acid means faster enamel breakdown.
Reduced saliva flow makes everything worse. Saliva washes away food debris, neutralizes acid, and delivers calcium and phosphate to remineralize enamel between meals. When dehydration from high blood sugar reduces flow, every one of those defenses weakens at the same moment that bacterial activity is rising. You get more attack and less defense in the same mouth.
The cavity burden tends to show up in places people do not expect. Adults with diabetes often see decay along the gumline and on root surfaces exposed by gum recession, areas that were stable for decades. Cavities between teeth also become more common because saliva is not flowing through those spaces to clear residue.
How Diabetes Tooth Decay Develops in the Mouth
Dry mouth is the single biggest contributor, which is why we cover it separately in our dry mouth causes and remedies guide. Without enough saliva, the mouth loses its natural rinse cycle, the chemistry tilts toward acid, and remineralization slows. Even people with otherwise excellent brushing habits can develop cavities under these conditions.
Glucose levels in saliva rise and fall with blood glucose, and the Journal of Dental Research has published studies tracking how elevated salivary glucose correlates with increased cavity-causing bacterial counts. This is part of why people who get their A1C back in range often report fewer dental problems even before they change their oral hygiene routine.
The immune response also weakens. White blood cells that normally help control bacterial colonies on tooth surfaces and in gum tissue become less efficient when blood glucose runs high. The National Institute of Dental and Craniofacial Research notes that this immune dampening is part of why people with diabetes face higher rates of multiple oral infections, not just cavities.
Gum recession exposes a more vulnerable surface. The crown of your tooth is covered in enamel, the hardest tissue in your body. The root, normally hidden under gum tissue, is covered only in cementum, which is much softer and dissolves more easily under acid attack. As gum disease and recession progress, more of that softer surface becomes exposed, and decay there moves fast.
The Gum Disease and Tooth Decay Overlap
Gum disease and cavities used to be treated as separate problems with separate causes, but they share more than people realize. Both are driven by bacterial colonies feeding on sugar, both worsen with reduced saliva, and both progress faster when the immune response is dampened. With diabetes, all three drivers tend to move in the wrong direction together.
Gum recession from periodontal disease creates the exposed root surfaces where root caries form, which is why people with both conditions often see clusters of new cavities at the gumline. Treating gum disease aggressively can slow that pattern by halting the recession before it exposes new surfaces. Our deeper guide on diabetes and gum disease prevention walks through the warning signs and treatment options.
The shared bacterial environment also matters. The same plaque biofilm that drives gingivitis and periodontitis is also the source of the acids that demineralize enamel. Disrupting that biofilm through good brushing, flossing, and professional cleanings cuts both risks at once. There is rarely a tradeoff between gum care and cavity care; they reinforce each other.
Treating one condition often helps the other. People who follow through on periodontal therapy, with deep cleanings, antimicrobial rinses, and tight home care, frequently see their cavity rate drop in parallel. The reverse is also true; aggressive cavity prevention with fluoride and sealants reduces the bacterial load that drives gum disease.
How to Prevent Tooth Decay When You Have Diabetes
Brushing technique is more important than brand. Use a soft-bristled brush at a 45-degree angle to the gumline, in short gentle strokes for two minutes total, twice a day. An electric brush with a pressure sensor and timer takes the variability out, especially helpful for people with neuropathy or arthritis. The American Dental Association keeps current guidance on technique and product selection.
Timing matters as much as technique. Brush before bed because saliva flow drops during sleep, leaving teeth more vulnerable to whatever is left on them. Wait at least 30 minutes after consuming acidic foods or drinks, including citrus, soda, and even some sports drinks, because brushing acid-softened enamel can wear it down faster.
Flossing reaches what brushing cannot. About 40 percent of tooth surfaces sit between teeth, and the gumline pockets where decay and gum disease both start are simply not accessible to a brush. Whether you use traditional floss, a water flosser, or interdental brushes is a matter of preference; doing it once a day is what counts.
Manage dry mouth proactively rather than waiting for cavities to confirm the problem:
- Sip water through the day to support saliva flow
- Chew xylitol gum after meals to stimulate saliva and reduce bacteria
- Use alcohol-free rinses designed for dry mouth
- Run a humidifier at night if mornings feel parched
Dietary choices that protect both teeth and blood sugar overlap significantly. Limit sticky carbohydrates like dried fruit and sweetened cereal that cling to enamel, pair carbs with protein or fat to slow glucose absorption and the time sugar sits on teeth, and rinse with water after eating anything sweet or acidic. None of these requires dramatic restriction, just a small shift in how you sequence and clean up after meals.
From my experience: Fourteen years into life with type 1, the year my numbers drifted up was also the year I got my first adult cavities. Two of them, in teeth that had been clean since childhood. I had not changed my diet or my brushing. What changed was my A1C creeping from the mid-six range into the low sevens, and the dry mouth that came with it. Tightening my management got my mouth back, no extra brushing required.
Dental Care That Targets Decay Prevention
In-office fluoride treatments give your enamel a measurable boost. A high-concentration fluoride varnish or gel applied every three to four months can offset much of the elevated cavity risk that comes with diabetes-related dry mouth. Some dentists prescribe custom fluoride trays for home use, delivering a higher dose than over-the-counter toothpaste.
Dental sealants are not just for kids. The deep grooves on adult molars trap food and bacteria in places brushing rarely reaches, and sealing those grooves with a thin protective coating can prevent decay before it starts. People with high cavity risk benefit from sealants well into adulthood.
More frequent professional cleanings catch problems earlier. Our dental care tips for people with diabetes guide covers the broader case for moving from a six-month recall to a three- or four-month interval, and decay prevention is one of the strongest reasons. If you are weighing replacement work, our piece on diabetes and dental implants explains how diabetes tooth decay history affects the planning conversation. Tartar that has been on a tooth for three months is far less destructive than tartar that has been there for six.
Choose oral care products with diabetes risk in mind. Look for fluoride toothpaste with at least 1,000 ppm fluoride, alcohol-free mouth rinses if you have any dry mouth, and a soft-bristled or electric brush. Skip whitening toothpastes that contain abrasives if your enamel is already compromised, and ask your dentist about prescription-strength fluoride if cavities keep appearing.
The Role of Dry Mouth in Tooth Decay
Saliva does more than keep your mouth comfortable. It buffers acid produced by oral bacteria, washes away residual food particles, and delivers minerals like calcium, phosphate, and fluoride that actively rebuild enamel between meals. When flow drops, every one of those protective functions weakens at once.
Diabetes tooth decay accelerates because the buffering system fails right when the bacterial load is rising. The pH of the mouth, which normally returns to neutral within 20 to 30 minutes after eating, can stay acidic for hours when saliva is reduced. That extended acid exposure is what drives the rapid decay people with poorly managed diabetes sometimes experience.
Home remedies that maintain moisture also protect teeth. Sipping water frequently, chewing sugar-free gum, using saliva substitutes before bed, and running a humidifier at night all support the natural defense system. Over-the-counter dry mouth products like Biotene and ACT Dry Mouth offer fluoride and moisturizing ingredients in one package.
If home remedies and OTC products are not enough, prescription saliva stimulants like pilocarpine and cevimeline may help. They work by directly stimulating the salivary glands and are especially useful when nerve damage or medication side effects are the main driver. Your dentist or doctor can review whether they are right for you based on your full medical history.
Frequently Asked Questions
Does diabetes increase the risk of tooth decay?
Yes. Diabetes promotes tooth decay through dry mouth, elevated glucose in saliva, impaired immune response, and gum recession that exposes softer root surfaces. Managing blood sugar steadily and maintaining good oral hygiene significantly reduce the elevated risk.
How to prevent tooth decay when you have diabetes?
Brush with fluoride toothpaste twice daily, floss every day, manage dry mouth proactively, visit the dentist every three to four months, and keep blood sugar in your target range as much as possible. The combination is what works; no single piece carries the whole load.
Why am I getting cavities even though I brush regularly?
When dry mouth and elevated salivary glucose are working against you, even good brushing may not be enough. Fluoride exposure, more frequent cleanings, dry mouth management, and blood sugar steadiness are usually the missing pieces. Talk to your dentist about prescription-strength fluoride if cavities keep appearing.
Can I reverse early tooth decay if I have diabetes?
Sometimes. Very early enamel demineralization, before a cavity forms, can sometimes be reversed with high-fluoride toothpaste, in-office fluoride treatments, and improved oral hygiene. Once a cavity has fully formed, it requires a filling, but stopping new ones is very possible.
Does sugar from food cause cavities, or is it the diabetes?
Both, and they amplify each other. Dietary sugar feeds cavity-causing bacteria, and diabetes creates the dry mouth and altered saliva chemistry that lets those bacteria do more damage. Reducing sticky sugar exposure and managing blood sugar together is more effective than either alone.
The real connection between diabetes tooth decay and your daily life comes down to a handful of mechanisms that all push in the same direction. Saliva, glucose, immune response, and gum health each play a role, and tightening all of them at once is the prevention strategy that works. Steady blood sugar, smart oral hygiene, and a dentist who knows your full picture give you the best shot at keeping the teeth you have for the long haul.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.