Diabetes with Chronic Kidney Disease: CKD Stages Explained
Diabetes with chronic kidney disease explained stage by stage, with eGFR ranges, symptoms, and what management looks like at each step from CKD 1 through.

In this article(11)
Learning that you have diabetes with chronic kidney disease can feel overwhelming, but understanding the CKD stages gives you a clearer picture of where you stand and what comes next. Each stage has its own management approach, and knowing what to expect at each point helps you plan ahead and stay engaged in your care.
The five-stage system used worldwide is based on a single number: your eGFR, which estimates how well your kidneys are filtering. Once you understand what that number means at each stage, the rest of the picture starts to click into place. We will walk through each stage with the practical details that matter, including what changes in your diabetes care along the way.
What Is Chronic Kidney Disease?
Chronic kidney disease (CKD) is the gradual loss of kidney function over time. The condition is defined either by reduced filtering capacity, measured by eGFR, or by signs of kidney damage like protein leakage that persist for at least three months. Most people with diabetes with chronic kidney disease are diagnosed through routine lab work rather than because of symptoms.
eGFR, or estimated glomerular filtration rate, comes from a blood creatinine test. The number is calibrated to roughly match how many milliliters of blood your kidneys can filter per minute, normalized to body size. A healthy young adult often has an eGFR above 100, and the National Kidney Foundation explains that eGFR naturally drifts down with age even without disease.
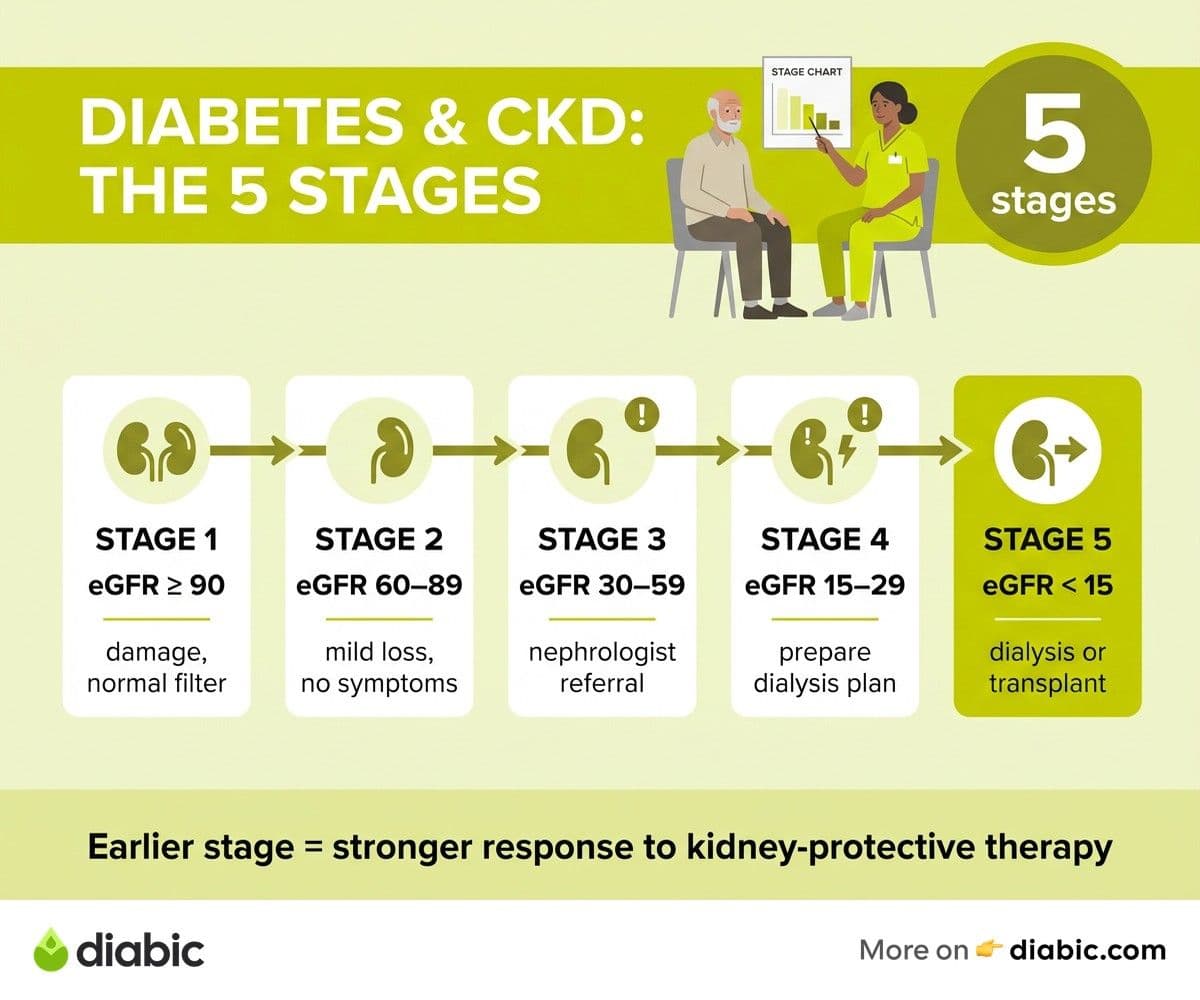
The five stages of CKD are based on eGFR ranges. Stage 1 means kidney damage with normal filtering; stage 5 means kidney failure. Each stage has implications for symptoms, monitoring, and treatment. Our broader diabetes with kidney disease guide covers the connection in more depth if you are new to this topic.
CKD is common in diabetes because high blood sugar damages the small filtering units (nephrons) inside the kidneys. The NIDDK reports that diabetes is the leading cause of CKD in the United States, ahead of high blood pressure and other conditions. The progression is usually slow, which means there is genuinely time to act.
CKD Stage 1: Kidney Damage with Normal Function
Stage 1 means your eGFR is 90 or above, but there are signs of kidney damage, most commonly protein in the urine. Filtering capacity looks normal on paper, yet something is happening structurally that the body wants you to know about.
Symptoms at stage 1 are essentially nonexistent. Most people learn about it from a routine UACR (urine albumin-to-creatinine ratio) test that catches protein leakage. This is exactly why annual screening matters in diabetes. You can read more about spotting diabetes kidney problems symptoms early if you want a deeper look at warning signs.
Management at this stage focuses on the basics: blood sugar within your target range, blood pressure under 130/80 for most people, and annual monitoring of eGFR and UACR. Some providers add an ACE inhibitor or ARB if protein leakage is present, even when blood pressure is normal, because these medications protect the kidneys directly.
Catching CKD at stage 1 offers the best long-term outcomes. With consistent management, many people stabilize here for years or even decades. The ADA emphasizes that early-stage interventions often slow or halt progression entirely.
CKD Stage 2: Mild Loss of Function
Stage 2 covers an eGFR between 60 and 89 with signs of kidney damage. Filtering has dipped slightly, but the change is mild enough that most people still feel completely fine.
Symptoms remain absent for nearly everyone. The main difference from stage 1 is that filtering has started to drop. Without protein leakage or another marker of damage, an eGFR in this range is not actually classified as CKD, since some decline is normal with age.
The management plan looks similar to stage 1, with continued focus on the same risk factors. Your provider may adjust medication doses, particularly metformin, depending on the trend in your eGFR. Some people start an SGLT2 inhibitor or finerenone at this stage if other risk factors are present.
Dietary adjustments are usually minor. Watching sodium, eating plenty of vegetables, and being mindful of ultra-processed foods is enough for most people at this point. Heavier protein restrictions and potassium or phosphorus tracking are not typically needed yet.
CKD Stage 3: Moderate Loss of Function
Stage 3 is where many people first hear "kidney disease" from their doctor. eGFR sits between 30 and 59 and is divided into two substages. Stage 3A is eGFR 45 to 59. Stage 3B is eGFR 30 to 44, which represents more meaningful loss.
Symptoms may start to appear at stage 3, though they are still subtle for many people. Fatigue, mild swelling in the ankles, changes in how often you urinate, or itchy skin can show up. Many people still feel normal, which is why lab values matter more than how you feel.
Medication adjustments often happen here. Metformin is still safe at most stage 3 levels but typically requires dose reduction once eGFR drops below 45. Some diabetes medications may need to change or be stopped. Insulin doses sometimes need to come down because the kidneys clear less of it as filtering slows.
Referral to a nephrologist usually happens at stage 3, especially stage 3B. A nephrologist will run more detailed tests, fine-tune kidney-protective medications, and watch your trends closely. Going to a kidney specialist does not mean things are dire, it means you are getting more focused care.
A 2020 analysis published in Diabetes Care found that the rate of eGFR decline can often be slowed substantially with the right combination of blood pressure control, kidney-protective medications, and metabolic management. We cover the full picture in our kidney disease treatment options post.
From my experience: my closest friend with type 2 diabetes was diagnosed at stage 3A after years of feeling fine. The first appointment with the nephrologist felt heavy, but by the third visit, his lab values had stabilized and his anxiety had dropped significantly. The plan is what made the difference, not the diagnosis label.
CKD Stage 4: Severe Loss of Function
Stage 4 means eGFR between 15 and 29. At this point, kidneys have lost a meaningful portion of their filtering capacity, and symptoms are usually more noticeable. Nausea, appetite changes, trouble concentrating, and fatigue often become harder to ignore.
This is the stage where preparation for what comes next becomes part of care. Your nephrologist will likely begin discussions about dialysis options or kidney transplant evaluation, even if you are not close to needing them yet. Early planning means you have time to ask questions, weigh options, and choose a path that fits your life.
Dietary restrictions become more important. Phosphorus, potassium, and protein need careful attention because the kidneys can no longer balance them well on their own. A renal dietitian becomes a key part of your team. Our kidney friendly diet for diabetes guide covers this transition in detail.
Diabetes management also changes. Many of the medications people relied on earlier are no longer appropriate. Insulin often becomes the primary treatment, and doses may need frequent adjustment because your body processes it differently. Hypoglycemia risk goes up, so checking blood sugar more often is usually recommended.
CKD Stage 5: Kidney Failure
Stage 5 is defined as eGFR below 15. At this point, the kidneys can no longer filter enough waste and fluid to sustain life on their own, and dialysis or a kidney transplant is needed. The phrase "kidney failure" sounds final, but stage 5 is also called end-stage renal disease, and many people live full lives on dialysis or with a transplant.
There are two main types of dialysis. Hemodialysis filters blood through a machine, usually three times a week at a clinic, though home hemodialysis is an option for some. Peritoneal dialysis uses the lining of your abdomen as a natural filter and is done at home, often overnight. The Mayo Clinic has a thorough breakdown of how each type works in practice.
Kidney transplant offers the best long-term outcomes for many people. The evaluation process can take months and includes a thorough review of cardiovascular health, infection risk, and other factors. Diabetes does not disqualify you from transplant, though it does shape how the team manages risk. Living-donor transplants generally have better outcomes than deceased-donor transplants, though both are common.
Living well at stage 5 is genuinely possible. Many people on dialysis continue to work, travel, and stay active. The transition is hard at first, but patient stories from the National Kidney Foundation show that quality of life often improves once a routine is established.
Managing Diabetes with Chronic Kidney Disease at Every Stage
Diabetes management itself shifts as CKD progresses. A1C targets, medication choices, and lifestyle priorities all change with kidney function.
Blood sugar targets are usually individualized rather than the standard "below 7%." Many people with stage 3 CKD or higher are kept slightly higher (between 7% and 8%) to reduce hypoglycemia risk. The kidneys clear insulin, and as they slow, low blood sugars become more common.
Medication safety is stage-dependent. Metformin works well in early stages but is restricted at lower eGFR values. SGLT2 inhibitors and finerenone are often added for kidney protection. GLP-1 receptor agonists are usually safe at most stages and have emerging kidney benefit data. The best diabetes medication for kidney disease post goes deeper on this question.
Coordinated care between your endocrinologist and nephrologist is one of the biggest factors in good outcomes. Bringing recent labs and a printed medication list to each appointment helps both specialists work from the same playbook.
Staying mentally and physically engaged matters at every stage. Walking, gentle strength training, time in community, and hobbies that give you a sense of normalcy all support resilience. CKD is something you live with, not something that defines your days.
Frequently Asked Questions
What are the CKD stages for people with diabetes?
CKD has five stages based on eGFR. Stage 1 (eGFR 90+) means kidney damage with normal function. Stage 2 (eGFR 60-89) is mild loss. Stage 3 (eGFR 30-59) is moderate loss, divided into 3A and 3B. Stage 4 (eGFR 15-29) is severe loss. Stage 5 (eGFR below 15) is kidney failure, requiring dialysis or transplant.
What happens at each stage of chronic kidney disease with diabetes?
Stages 1 and 2 usually have no symptoms; management focuses on blood sugar, blood pressure, and annual monitoring. Stage 3 may bring fatigue, swelling, and medication adjustments. Stage 4 brings more noticeable symptoms and preparation for advanced treatment. Stage 5 requires dialysis or transplant. Diabetes management adjusts at each stage to reduce hypoglycemia risk and protect remaining kidney function.
Can CKD progression be slowed in people with diabetes?
Yes, in many cases. Tight blood pressure control, ACE inhibitors or ARBs, SGLT2 inhibitors, and consistent blood sugar management can slow or stop progression for years. Research suggests that early intervention at stages 1 to 3 produces the strongest results. Talk to your doctor about whether kidney-protective medications fit your situation.
Living with diabetes with chronic kidney disease is a long game made up of small, repeatable habits. Track your eGFR, keep your appointments, ask questions about every medication change, and lean on your care team as the picture evolves.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.