Insulin Therapy for Type 1 Diabetes Explained
Insulin therapy for type 1 diabetes can feel overwhelming. This practical guide covers insulin types, delivery methods, dosing, and daily management.

In this article(10)
Insulin therapy for type 1 diabetes is not optional; it is the foundation of survival and daily management. Yet the number of insulin types, delivery methods, and dosing strategies can feel overwhelming, especially in the first weeks after diagnosis when every meal feels like a math problem.
This guide walks through how insulin therapy actually works in practice, not just in theory. We cover the types of insulin commonly prescribed, the different ways to deliver it, how doses get calculated, and the real-world challenges that come with the territory.
The goal is not to replace your endocrinologist or diabetes educator. The goal is to help you walk into those appointments with better questions and a clearer picture of what to expect.
How Insulin Therapy for Type 1 Diabetes Works
In type 1 diabetes, the immune system has destroyed the beta cells in the pancreas, the tiny factories responsible for producing insulin. Without insulin, glucose cannot move from the bloodstream into cells where it is needed for energy. The body essentially starves while blood sugar climbs to dangerous levels, which is why type 1 diabetes symptoms like rapid weight loss and extreme thirst show up so quickly.
Insulin therapy replaces what the pancreas can no longer make. The challenge is that a healthy pancreas releases insulin in a beautifully responsive way: a steady background drip throughout the day and night, plus precise bursts when food enters the system. Replicating that with injections or a pump takes practice and constant fine-tuning.
Most modern insulin therapy follows a basal-bolus approach. Basal insulin provides the steady background coverage your body needs between meals and overnight. Bolus insulin is taken before meals to handle the rise in blood sugar from carbohydrates, and as a correction when blood sugar runs high. The NIDDK guide to insulin medicines and treatments breaks down these categories in clinical detail.
Matching insulin to food, activity, stress, and sleep is the daily art of type 1 management. No two days are identical, and your needs will change with illness, hormones, exercise, and even the weather. Flexibility is part of the design.
Types of Insulin Used in Type 1 Diabetes
Insulin comes in several forms, each with a different onset, peak, and duration of action. Most people with type 1 use a combination of two or more types, prescribed by a care team that knows their patterns. Here is a quick overview of the main categories.
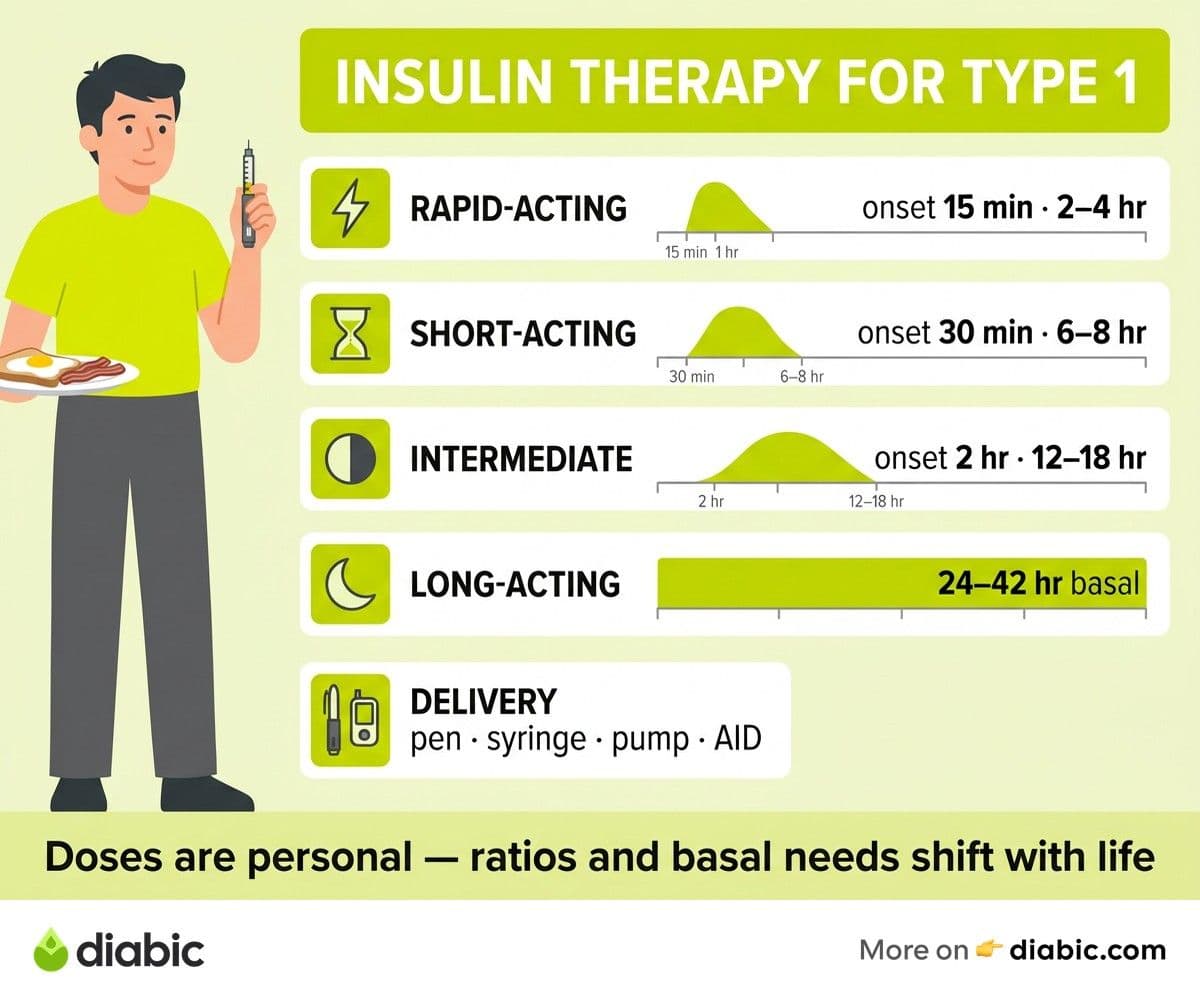
Rapid-acting insulin starts working within about 15 minutes, peaks around one hour, and lasts roughly two to four hours. Common brand names include lispro (Humalog), aspart (NovoLog, Fiasp), and glulisine (Apidra). This is the workhorse for mealtime dosing and corrections.
Short-acting (regular) insulin takes about 30 minutes to start working and lasts up to six to eight hours. Once standard for mealtime dosing, it has largely been replaced by rapid-acting insulin in most modern care plans, though it still has uses.
Intermediate-acting insulin like NPH starts working within about two hours and lasts 12 to 18 hours. It used to be a common basal option but is less popular today because of its peak, which can cause unexpected lows.
Long-acting insulin provides the steady basal coverage. Glargine (Lantus, Basaglar, Toujeo), detemir (Levemir), and degludec (Tresiba) are the most common. Degludec lasts more than 42 hours, giving the most flexible dosing window of the group.
Pre-mixed insulin combines rapid or short-acting with intermediate-acting in a fixed ratio. These are less commonly used in type 1 because they offer less flexibility for adjusting doses around meals and activity.
The American Diabetes Association's insulin guide explains how each type fits into modern care. If you are still getting up to speed on the condition itself, our explainer on what is type 1 diabetes covers the autoimmune basics and how diagnosis typically unfolds.
Insulin Delivery Methods
How you take insulin matters almost as much as which insulin you take. Each method has tradeoffs, and the right fit depends on lifestyle, dexterity, insurance coverage, and personal preference.
Syringes and vials are the original delivery method and still widely used. They are inexpensive, portable, and require no batteries. Drawing up a precise dose takes practice but is straightforward once learned.
Insulin pens come in prefilled or reusable cartridge form. Most people find pens easier to carry, more discreet to use in public, and more accurate for small doses. Smart pens that record dose timing and amount through a connected app are also becoming more common.
Insulin pumps deliver rapid-acting insulin continuously through a thin tube and small cannula inserted under the skin, replaced every few days. They allow for more flexible dosing and can adjust delivery in tiny increments throughout the day. Pumps require commitment to learning the system and managing the wearable hardware.
Automated insulin delivery (AID) systems, sometimes called hybrid closed-loop or "artificial pancreas" systems, pair a pump with a continuous glucose monitor (CGM). The system automatically adjusts background insulin delivery based on real-time glucose readings. Mealtime boluses still require user input, but overnight management has improved dramatically for many users.
Inhaled insulin (Afrezza) is a rapid-acting option taken through an inhaler before meals. It is faster-onset than injected insulin for some people but is not appropriate for everyone, especially those with lung conditions. Breakthrough T1D's administering insulin guide provides a useful comparison of these delivery methods in practice.
Getting Your Doses Right
Dosing is where insulin therapy gets personal. There is no universal formula because every body responds differently to food, exercise, stress, and sleep. Most people work with their care team to develop two key personalized numbers.
The first is the insulin-to-carbohydrate ratio, which tells you how many grams of carbs are covered by one unit of insulin. A ratio of 1:10, for example, means one unit covers ten grams of carbs. Counting carbs accurately becomes a daily skill.
The second is the correction factor (or insulin sensitivity factor), which estimates how much one unit of insulin will lower your blood sugar. If your correction factor is 50, one unit drops your blood sugar by about 50 mg/dL. Together, these numbers help calculate how much insulin to take for a given meal or high reading.
Basal rates matter too. With long-acting insulin, you typically take one or two doses per day. With a pump, basal rates can be programmed to vary by hour, accommodating the dawn phenomenon (a natural blood sugar rise in early morning) or activity patterns. Adjusting basal needs requires testing and patience, often guided by your care team.
Doses change over time. Puberty, pregnancy, weight changes, illness, exercise routines, stress levels, and even seasonal shifts can all affect insulin needs. Your starting doses are not your forever doses. The Mayo Clinic's type 1 treatment overview reinforces that dosing is an ongoing conversation with your provider, not a one-time prescription.
From my experience: when I was first diagnosed at twelve, my insulin-to-carb ratio was 1:25 because my honeymoon phase still left some pancreas function. Within two years it dropped to 1:8. Then in my twenties, after I started lifting weights regularly, my basal needs dropped by almost a third. Now in my mid-thirties, I check my settings every six months because they keep shifting. The biggest lesson fourteen years in: assume your body is going to change, and treat your doses as a living document, not a verdict.
Common Challenges and How to Handle Them
Insulin therapy comes with real challenges, and pretending otherwise does no one any favors. Knowing what to expect makes them easier to manage when they show up.
Low blood sugar (hypoglycemia) is the most immediate risk of insulin therapy. Taking too much, eating less than expected, or unplanned activity can all push blood sugar dangerously low. Symptoms include shakiness, sweating, confusion, and fast heartbeat. Knowing the low blood sugar symptoms and keeping fast-acting glucose nearby is essential. Severe lows require glucagon and emergency response.
Injection site rotation matters more than people realize. Repeatedly injecting in the same spot can cause lipodystrophy, where fatty tissue under the skin thickens or shrinks, making insulin absorption unpredictable. Rotating between abdomen, thighs, upper arms, and buttocks helps keep tissue healthy.
Insulin stacking happens when you take a correction dose before previous insulin has finished working, leading to cumulative drops and unexpected lows. Most CGMs and smart pens now warn about active insulin on board, but the principle takes time to internalize.
Decision fatigue is the part nobody warns you about. Type 1 demands hundreds of small choices a day, and that cognitive load is real. Building routines, automating what you can, and giving yourself permission to have imperfect days is part of sustainable management. Our piece on living with type 1 diabetes digs into this side of life with the condition. We also have an honest look at diabetes insulin myths for anyone tired of misinformation from well-meaning friends and family.
FAQ
How does insulin therapy work for type 1 diabetes?
In type 1 diabetes, the immune system destroys the insulin-producing beta cells in the pancreas, so the body needs external insulin to survive. Insulin therapy typically combines a long-acting insulin for baseline (basal) needs with a rapid-acting insulin before meals (bolus). The goal is to mimic the body's natural insulin release as closely as possible, matching insulin to food, activity, and blood sugar levels throughout the day.
What types of insulin are used for type 1 diabetes?
The most common types include rapid-acting insulin like lispro, aspart, and glulisine for mealtime dosing, and long-acting insulin like glargine, detemir, and degludec for background coverage. Some people use insulin pumps that deliver rapid-acting insulin continuously, eliminating the need for separate long-acting injections. Your care team selects the combination based on your lifestyle, blood sugar patterns, and personal preferences.
Can you live a normal life with insulin therapy?
Yes. With modern insulin, delivery technology, and continuous glucose monitoring, people with type 1 diabetes pursue careers, athletics, parenthood, and travel just like anyone else. Daily management is real, but it does not have to define your life. Most people find that the early learning curve gives way to a routine that becomes second nature.
Do you need insulin forever with type 1 diabetes?
Yes. Type 1 diabetes is currently a lifelong condition with no cure, and insulin replacement is essential. Research into beta cell transplants, immune-modulating therapies, and stem cell treatments is active, but for now, insulin remains the foundation of care. Talk to your doctor about clinical trials if you are interested in emerging options.
Insulin therapy for type 1 diabetes is demanding, but it is also a remarkable medical achievement. Each dose is a small act of stepping in for a body that needs help, and over time, that act becomes part of who you are without overshadowing everything else. The technology keeps improving, the community keeps growing, and the day-to-day side of insulin therapy for type 1 diabetes gets more manageable than it feels in the first overwhelming weeks.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Diabetes Knowledge
View all
Small Lifestyle Changes for Prediabetes, Big Results
A small lifestyle change for prediabetes, done consistently, can rival medication. Here is what actually works and how to build habits that stick.

Low Blood Sugar Symptoms That Hit Without Warning
Learn the low blood sugar symptoms that strike without warning, how to respond fast with the ADA Rule of 15, and when to call for help.

Weight Loss for Prediabetes: A Realistic Approach
Weight loss for prediabetes does not require extreme dieting. Learn the 5-7% target, what works, and how to set realistic, sustainable goals.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.