Diabetic Foot Ulcer Treatment and Prevention
Diabetic foot ulcer treatment works best when started early. Learn how ulcers are treated, why they form, and the daily steps that prevent them.

In this article(10)
A small blister you barely felt yesterday looks angrier this morning. The skin around it is pinker than expected, and there is a faint shine that was not there before. For people with diabetes, that quiet shift can be the start of a foot ulcer, and the next 48 hours often shape the outcome. Diabetic foot ulcer treatment is most effective when it begins early, and prevention is more powerful still.
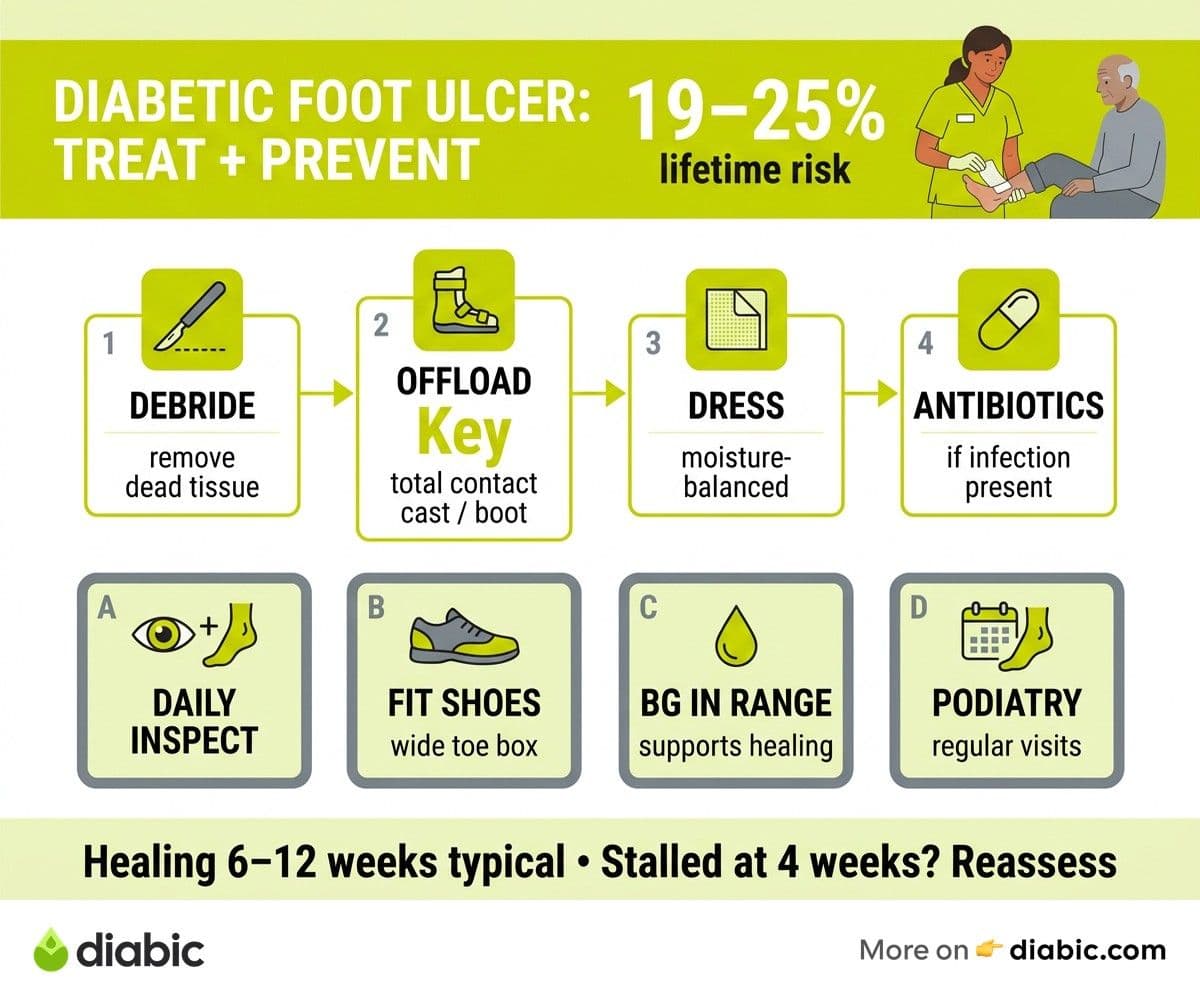
Foot ulcers affect roughly 19 to 25 percent of people with diabetes at some point in their lives, according to data summarized by the ADA's foot complications guidance. Most ulcers are preventable, and most that do form can be healed with the right combination of care, time, and attention. This guide walks through what treatment looks like, why ulcers form in the first place, and how to keep your feet on the safer side of those statistics.
How Diabetic Foot Ulcer Treatment Works
Diabetic foot ulcer treatment usually begins with debridement, the removal of dead or unhealthy tissue from the wound. A clinician uses a scalpel, special instruments, or a specialized dressing to clear debris so that healthy tissue underneath can begin to grow. Debridement may be repeated several times across visits, since fresh tissue exposure is one of the strongest drivers of healing.
Offloading is the next pillar, and it is often what determines whether an ulcer heals or stalls. Walking on an ulcer reinjures it with every step, so the goal is to remove pressure entirely from the wound. Total contact casts, removable cast walkers, and specialized offloading boots redistribute weight so the ulcer can rest. Wound dressings then keep the environment moist enough to support tissue growth without becoming wet enough to encourage infection. Antibiotic therapy is added when infection is present, guided by the depth of the wound and any cultures taken. The Wound Healing Society resources on diabetic ulcer care describe a stepwise approach, with advanced options like skin grafts, growth factors, bioengineered skin substitutes, and hyperbaric oxygen reserved for wounds that do not respond to standard care. For wound healing support outside the clinic, our notes on supporting diabetic wound healing at home cover the daily habits that complement medical treatment.
Can Diabetic Foot Ulcers Be Prevented
In many cases, yes. The NIDDK guidance on preventing diabetic foot complications frames prevention as a daily practice rather than a one-time fix. A short foot inspection each evening, ideally paired with another routine like brushing your teeth, catches blisters, redness, and small cuts before they progress. Use a handheld mirror or your phone camera to see the bottoms and sides of your feet.
Footwear is the second piece. Shoes that fit properly, with a wide toe box, seamless interior, and cushioned sole, eliminate many of the pressure points that turn into ulcers. People with high-risk feet may qualify for therapeutic footwear through Medicare, fitted by a podiatrist or pedorthist. Replacing shoes before they pack down or rotate is part of preventing recurrence, not just initial ulcers.
Blood sugar management supports both prevention and healing. The closer your numbers stay to your target range, the better your tissue oxygenation, immune response, and wound repair work. Regular podiatric visits add a professional set of eyes to the equation. A podiatrist can identify calluses, deformities, and pressure patterns long before they break the skin, and they can address those issues with trimming, padding, or referral. Pair these habits with a structured diabetic foot care and prevention guide so prevention does not depend on memory alone.
Understanding Diabetic Foot Conditions
A diabetic foot ulcer is an open sore that forms on the foot and fails to heal in the normal timeframe due to underlying diabetes-related changes. Most ulcers form on weight-bearing surfaces: the ball of the foot, the big toe, the heel, or the side of the foot where shoes rub. They begin as small breaks in the skin from friction, pressure, or a tiny puncture, then deepen because the body cannot close them quickly.
Two factors create the conditions that allow ulcers to form. Peripheral neuropathy reduces sensation, so a person may walk on a stone in their shoe, a hot surface, or a developing blister without feeling pain. Peripheral arterial disease narrows the small vessels that feed the foot, slowing tissue repair and reducing the immune cells that reach a fresh wound. Together, neuropathy and reduced blood flow create the perfect setup for a small injury to become a chronic ulcer.
Clinicians grade severity using the Wagner classification system, which ranges from Grade 0 (high-risk foot with no open ulcer) to Grade 5 (extensive gangrene requiring amputation). Most ulcers seen in primary care fall in Grades 1 to 3, where the wound is open but has not spread to bone or extensive infection. Knowing the grade helps your team match treatment to severity, and early-stage ulcers respond far better than later ones.
Diabetic Wound Healing Challenges
Diabetes affects nearly every step of the healing cascade. High blood sugar slows white blood cell function, making infections more likely and harder to clear. It also stiffens the small blood vessels that deliver oxygen and nutrients to the wound bed, creating a slow trickle where a strong flow is needed. Inflammation, normally a short and intense phase, can become prolonged, leaving the wound stuck in a state of low-grade injury.
Blood sugar at the time of injury and during healing matters. Several studies referenced in ADA materials show that wounds heal faster when A1C is closer to target and daily glucose stays in range. Nutrition plays a role too. Adequate protein, vitamin C, zinc, and hydration give the body the building blocks for new tissue. Skipping meals or eating very low-protein for stretches of time can stall a wound.
Some ulcers heal slowly or recur because the underlying pressure pattern was never fixed. If a callus rebuilds in the same spot, the same pressure point will break down again. Recurrence is common after the first ulcer, which is why aftercare and footwear changes are as important as the initial healing. A wound that has not improved in four weeks deserves reassessment, often with imaging to rule out bone involvement.
Recognizing Foot Infection Symptoms with Ulcers
Infection changes the timeline for treatment. Watch for redness that spreads beyond the wound edges, increased warmth, swelling, new or worsening pain, and any drainage that is cloudy, yellow, green, or foul-smelling. A red streak running up the foot or leg, or fever and chills, signals that infection may be reaching deeper tissues or the bloodstream and needs urgent attention.
Some signs are subtler in people with neuropathy. You may not feel pain that would normally drive someone else to the clinic. Look for changes you can see and smell rather than relying on what you feel. The wound might also start producing more drainage or develop a darker, soft area at its edge. Trust your eyes when your feet cannot tell you the full story.
If you suspect infection, contact your healthcare team the same day. Treatment shifts to include antibiotics, sometimes intravenous if the infection is deep, and the wound care plan often becomes more intensive. Our deeper notes on diabetic foot infection symptoms can help you recognize the patterns earlier.
From my experience: After 14 years with type 1 diabetes, the closest call I had with a foot wound came from a barely visible scrape from a pool deck. I cleaned it, covered it, and assumed it was nothing. By day three the area was warm and pinker than it should have been. I called my podiatrist, started a short course of antibiotics, and it healed cleanly. The lesson stayed with me. Calling on day three rather than day seven probably saved me weeks of treatment.
Long-Term Prevention Strategies
A reliable foot care routine is the single biggest factor in preventing recurrence. Inspect your feet daily, wash and dry them gently, moisturize the tops and bottoms (not between toes), and trim nails straight across. If you cannot see your feet clearly, ask a partner or use a phone camera. Build the routine into a time you already protect, like right before bed.
Therapeutic footwear is worth wearing consistently, not just for special outings. Many people pull their good diabetic shoes out for appointments and revert to old sneakers around the house. The home is where most foot injuries start, so house shoes with proper support belong in the rotation too. Replace shoes when the cushioning packs down or the lining starts to fray.
Manage blood sugar steadily, schedule regular foot exams (at least once a year, more often if you are higher risk), and address calluses, hammertoes, or other deformities before they cause ulcers. Calluses can be safely shaved by a podiatrist, who can also fit padding or recommend orthotics. The goal is not perfection but a long, low-drama relationship with your feet.
Frequently Asked Questions
How are diabetic foot ulcers treated?
Treatment includes debridement to remove dead tissue, offloading to remove pressure from the wound, moisture-balanced dressings, and antibiotics if infection is present. Advanced cases may require skin grafts, growth factors, or hyperbaric oxygen therapy. Steady blood sugar management supports healing throughout the process.
Can diabetic foot ulcers be prevented?
In most cases, yes. Daily foot inspections, well-fitting shoes with a wide toe box, blood sugar management close to your target range, and regular podiatric checkups significantly reduce the risk. Addressing calluses and pressure points early stops many ulcers before they form.
How long does it take a diabetic foot ulcer to heal?
Healing time varies with the depth, location, and grade of the ulcer, plus blood sugar levels and circulation. Many uncomplicated ulcers heal in 6 to 12 weeks with consistent offloading and dressing changes. Deeper or infected ulcers can take several months. A wound that has not improved in 4 weeks should be reassessed by your provider.
If your feet need more attention than they have been getting, talk to your doctor or podiatrist about how diabetic foot ulcer treatment and a daily prevention routine fit your specific risk profile. Pair their guidance with the small home habits in this guide and check in regularly so any change is caught early.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.