Metformin Side Effects: What to Expect Week by Week
A clear look at metformin side effects, why they happen, how long they last, and what to do when your stomach pushes back against a new prescription.

In this article(13)
You filled the prescription, took the first pill with breakfast, and by mid-morning your stomach feels like it belongs to someone else. The bottle came with a long pamphlet, your search history is now full of worst-case scenarios, and you are wondering whether you should keep going. We hear this story almost every week from people just starting treatment for type 2 diabetes or insulin resistance.
Metformin side effects are the single most common reason people hesitate to stick with this medication, even though it has been a first-line therapy for decades. The good news is that most of what you experience in the first few weeks is predictable, manageable, and usually temporary. We want to walk you through what is normal, what is not, and how to make the early adjustment period easier on your body.
What Metformin Is and Why It Is Prescribed
Metformin belongs to a class of medications called biguanides, and the question of what is metformin really comes down to a single sentence: it is a glucose-lowering pill that works mostly by changing how your liver behaves. According to the American Diabetes Association Standards of Care, metformin remains the recommended first-line oral medication for most people with type 2 diabetes. It is also widely prescribed for prediabetes, polycystic ovary syndrome, and gestational diabetes follow-up care.
The drug has a long safety record, a low cost, and a mechanism that does not push your pancreas to make more insulin. That last point matters because it means metformin rarely causes hypoglycemia on its own, unlike some older diabetes medications. If you want a wider view of how it fits into a treatment plan, our overview of type 2 diabetes treatment options places metformin alongside the other tools your provider may consider.
Common Metformin Side Effects
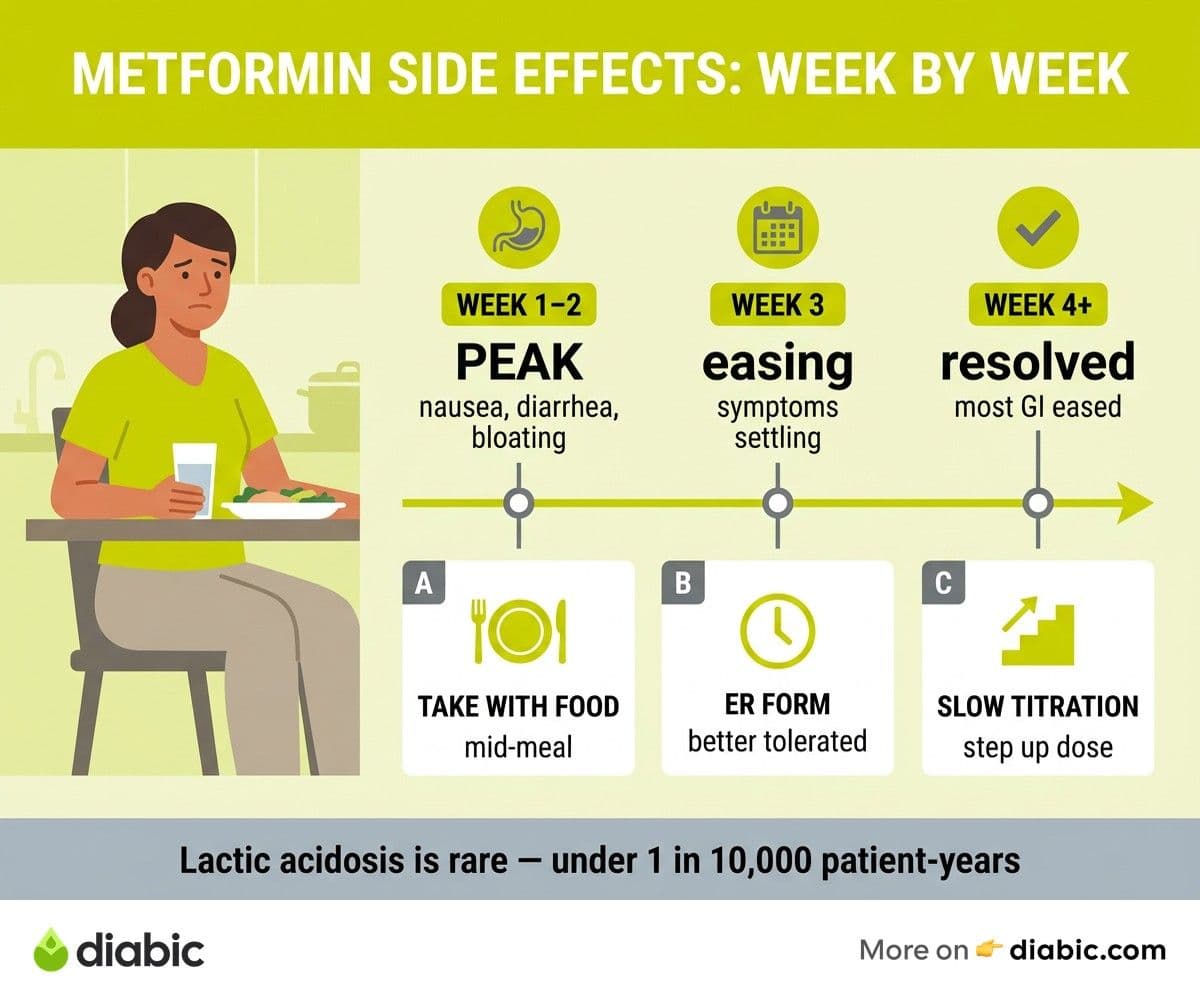
Most side effects from metformin land in your gut. The usual lineup includes nausea, diarrhea, stomach cramps, bloating, gas, and occasionally a mild metallic taste in the mouth. These tend to peak in the first one to two weeks after starting the medication or after any dose increase, and they often improve significantly by week four.
The reason your digestive system reacts is that metformin changes how glucose is absorbed in the small intestine and shifts the makeup of your gut bacteria. Your microbiome is not used to the new chemistry, and it complains in the form of urgency and discomfort. Some people also notice a temporary drop in appetite, which can feel disorienting if you are used to eating on a regular schedule. We have written more about this appetite shift in our piece on metformin and weight loss, since the two often show up together.
Bloating and gas tend to ease as your gut adapts, especially if you avoid sudden swings in your fiber intake during the first month. Diarrhea is the most disruptive symptom for many people, and it deserves its own conversation with your provider if it lasts more than a few weeks. Persistent gut symptoms are not something you have to white-knuckle through, even though they are technically considered common.
How to Manage Side Effects of Metformin
Small changes in how you take the medication can make a real difference. Taking metformin with food, ideally toward the middle or end of a meal rather than on an empty stomach, slows absorption and softens the digestive impact. Plain water alongside the dose helps too, and some people find that splitting their daily intake across two meals is gentler than a single larger dose.
The NICE guideline NG28 recommends slow titration, meaning your provider starts you on a low dose and steps up gradually over several weeks. This is one of the most evidence-backed strategies for reducing GI side effects, and it is worth asking about if you were started at a higher dose right away. Talk to your doctor about whether a slower ramp would work for you.
Switching from immediate-release metformin to extended-release, often listed as metformin ER or metformin XR, helps many people who cannot tolerate the standard form. The extended-release version delivers the medication more steadily, which usually means less stomach turbulence. It is the same medication at the same total daily amount, just packaged in a way that drips into your system more slowly.
When to call your provider
If side effects are interfering with eating, hydration, work, or sleep after the first two to three weeks, that is a reason to pick up the phone. The same goes for any symptom that feels new or unusual rather than typical digestive complaints. Your healthcare team would much rather hear about a problem early than have you stop the medication on your own.
Serious Side Effects That Need Medical Attention
Most metformin side effects are uncomfortable but not dangerous. There is, however, a short list of serious effects that warrant immediate medical attention. Lactic acidosis is extremely rare, with rates well under one in ten thousand patient-years according to studies summarized in Diabetes Care, but the symptoms are worth memorizing. They include unusual muscle pain, trouble breathing, persistent stomach pain with vomiting, extreme tiredness, and a slow or irregular heartbeat.
Lactic acidosis becomes more likely when kidney function drops, which is why your provider checks your kidney labs at least once a year. People with significantly reduced kidney function may need a different medication entirely, and our look at diabetes medication options for kidney disease explains how these decisions get made. Acute illness, dehydration, or contrast dye for imaging studies can also stress the kidneys temporarily, so let any treating physician know you take metformin before procedures.
Vitamin B12 deficiency is the other long-term concern worth knowing about. Studies in the BMJ have shown that long-term metformin use can lower B12 levels in a meaningful percentage of patients, and the deficiency can mimic neuropathy with tingling or numbness in the hands and feet. Many providers now check B12 levels every year or two and recommend supplementation when needed. Severe allergic reactions are rare but possible, and any sudden rash, swelling, or trouble breathing after a dose should be treated as an emergency.
What Does Metformin Do Inside Your Body
If you want to understand why the side effects show up where they do, it helps to know what does metformin do at a mechanical level. The medication works in three main places. It tells your liver to release less stored glucose into the bloodstream, especially overnight, which is why fasting blood sugars often improve first.
Metformin also makes your muscle and fat cells more responsive to insulin, so the insulin you already produce works harder. This insulin-sensitizing effect is part of why the medication is widely prescribed for metformin for insulin resistance even outside of formal type 2 diabetes diagnoses. Finally, it changes glucose handling in the gut itself, which is the piece most directly tied to the digestive side effects.
What metformin does not do is force your pancreas to make more insulin. That is a meaningful difference from medications like sulfonylureas, and it explains the relatively low rate of hypoglycemia when metformin is taken alone. Combined with other diabetes medications, the hypoglycemia picture changes, which is why your provider reviews your full medication list at every appointment.
Who Is Most Likely to Experience Side Effects
Not everyone reacts to metformin the same way. People starting at higher doses, people who skip the slow titration step, and people with existing GI conditions like irritable bowel syndrome tend to report more digestive symptoms. Body size, age, and overall gut health all play a role, although it is hard to predict in advance who will sail through and who will struggle.
Women taking metformin for PCOS sometimes notice that side effects feel different than what they expected from diabetes-focused information online. The dose ranges and goals can vary, and the management strategies do too. If you are taking metformin for PCOS, fertility support, or prediabetes rather than established type 2 diabetes, ask your provider how your situation might shape the side effect picture.
Kidney function is the single biggest factor in how well your body tolerates metformin over time. As kidneys filter the medication out of your system, slower clearance can mean higher blood levels and more side effects. Annual lab monitoring catches changes early, and dose adjustments based on those labs keep the medication working safely.
Long-Term Safety of Metformin
Metformin has been in use since the late 1950s, which makes it one of the most studied medications in modern medicine. Decades of follow-up data show that for most people, the long-term safety profile holds up well. Some studies suggest possible cardiovascular benefits beyond glucose lowering, although the evidence varies by population and trial design.
The main long-term considerations are the B12 monitoring already mentioned and ongoing checks of kidney function. Some people stay on metformin for decades, while others move to combination therapy or different medications as their diabetes evolves. Newer drug classes have arrived in recent years, but metformin remains a foundation in many treatment plans because it is effective, affordable, and well understood.
Your relationship with the medication is not static. Regular check-ins with your provider help you decide whether the dose is still right, whether labs are stable, and whether anything else in your health picture suggests a change. Managing your diabetes is an ongoing process, and the medications that work today may shift as your needs do.
Frequently Asked Questions
What are the most common side effects of metformin?
The most frequent reactions to this medication are gastrointestinal, including nausea, diarrhea, stomach cramps, bloating, and gas. Some people also notice a metallic taste or a mild drop in appetite. These symptoms are most pronounced in the first one to two weeks of treatment and after any dose increase.
Do metformin side effects go away over time?
For most people, yes. Digestive symptoms typically diminish significantly within two to four weeks as your body adjusts to the medication. If side effects persist or feel severe, talk to your healthcare provider about taking the medication with food, slowing the titration schedule, or switching to an extended-release formulation.
Can I stop taking metformin if I feel sick?
Do not stop the medication on your own without talking to your provider, even if you feel rough. Many side effects improve with timing changes or a switch to extended-release, and stopping abruptly can affect your blood sugar. Reach out, describe what you are experiencing, and decide together on the next step.
How long does it take for metformin to start working?
You may see fasting blood sugar improvements within a week, but the full effect on average glucose usually takes four to six weeks. Your provider will recheck your labs after a couple of months to see how your numbers have shifted and whether any dose changes make sense.
We hope this look at metformin side effects gives you a clearer sense of what to expect and where to push back when something feels off. Most people land on a comfortable routine within a month or two, and the rough early days fade into the background. If you are still in that early stretch, give yourself credit for sticking with a medication that takes some patience, and keep your provider in the loop along the way.
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Treatment & Medication
View all
Insulin Resistance Treatment Options Explained
Insulin resistance treatment is more than one pill. Here is a clear look at lifestyle, medication, and supplement options that actually work.

Insulin Resistance Diet: What to Eat and Avoid
An insulin resistance diet that fits real life. We cover foods that help, foods to limit, and meal patterns that improve insulin sensitivity.

Is Zepbound a Diabetes Medication? What You Need to Know
Is Zepbound a diabetes medication? We break down the FDA approval, the Mounjaro connection, and what tirzepatide means for blood sugar.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.