Best Diabetes Medication for Kidney Disease
Find the best diabetes medication for kidney disease, from kidney-protective SGLT2 inhibitors and GLP-1s to safe metformin dosing at low eGFR.

In this article(13)
Picking the best diabetes medication for kidney disease is no longer just about lowering blood sugar. The medication that fits you also has to protect a pair of organs already under strain, and that single decision can change how your kidney function tracks over the next decade. The newer class of glucose-lowering drugs has shifted what "best" actually means for someone living with both conditions.
If you have type 2 diabetes and chronic kidney disease (CKD), your medication list is doing two jobs at once. It is keeping glucose in a safer range while also influencing how fast your kidneys lose function over time. The goal of this guide is to help you walk into your next appointment with sharper questions, not a self-prescribed plan.
We will look at the medications that come up most often in current kidney guidelines, explain what the major trials actually showed, and flag what changes as your estimated glomerular filtration rate (eGFR) drops. Your nephrologist and endocrinologist remain the people who put it all together for your specific situation.
Why Medication Choice Matters for Kidney Health
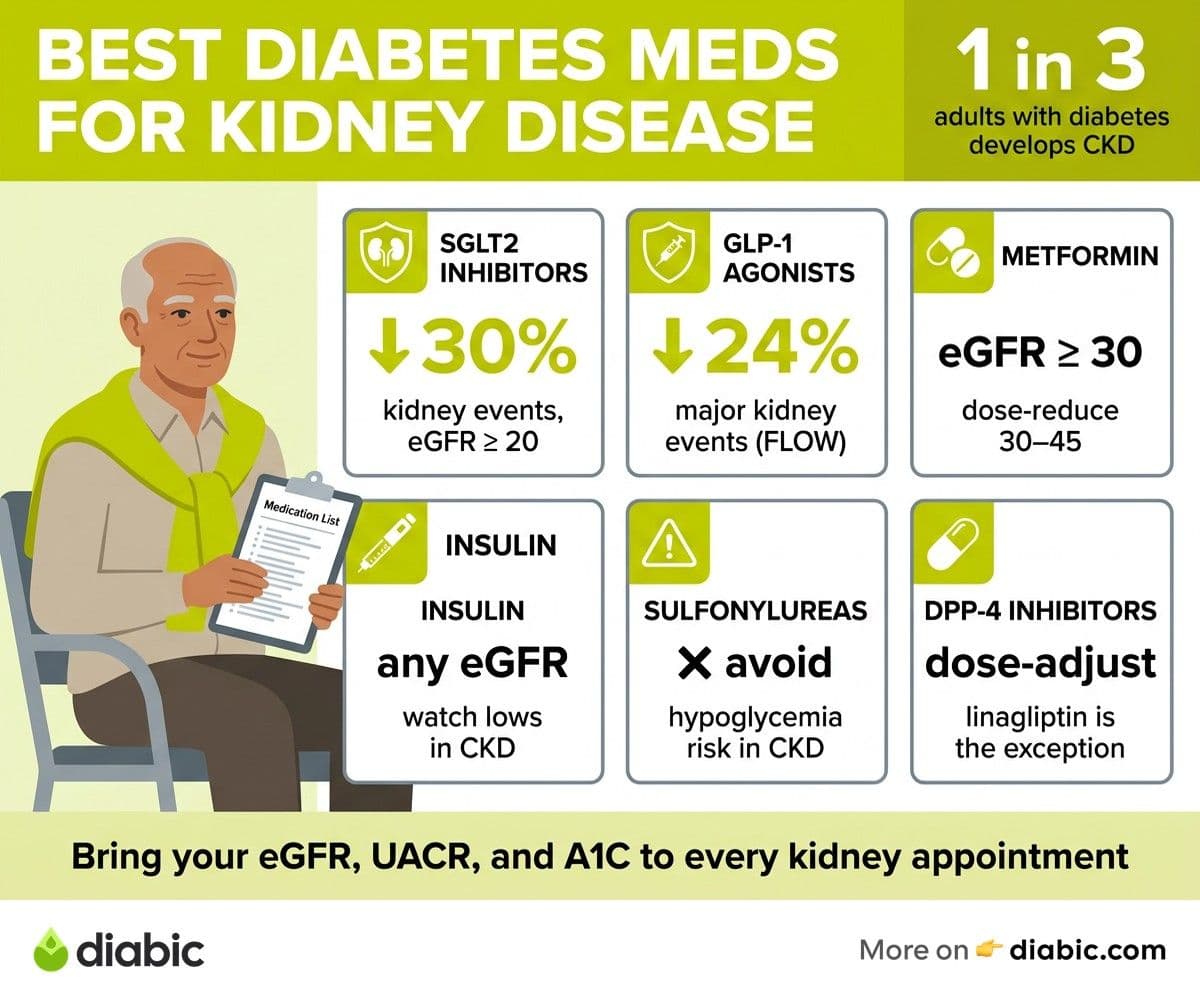
About one in three adults with diabetes develops some degree of kidney disease, according to the Centers for Disease Control and Prevention. That makes diabetes the leading cause of kidney failure in the United States. The medications you take influence not only your A1C but also the proteins leaking through your kidneys' filters and the rate at which those filters scar over.
Two things have changed in the last decade. First, several diabetes medications now have evidence that they slow the progression of kidney disease independent of their glucose-lowering effect. Second, older rules about which drugs were "off-limits" once kidney function declined have been rewritten as newer data has come in. The American Diabetes Association's Standards of Care now treats medication selection in CKD as a separate clinical decision, not an afterthought.
That is why a thoughtful conversation about your kidney disease treatment options belongs at every visit, especially when your eGFR or urine albumin numbers shift. The right drug for someone with an eGFR of 60 may not be the right drug a few years later at an eGFR of 35. If you want context on staging, our overview of diabetes with kidney disease walks through how clinicians track CKD over time.
SGLT2 Inhibitors: The Best Diabetes Medication for Kidney Disease in Most Cases
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are the medications that reshaped how doctors think about diabetes medication for kidney disease. They block a transporter in the kidney that normally reclaims glucose, so excess glucose is excreted in urine. That mechanism alone lowers blood sugar, but the kidney-protective effects appear to come from changes in pressure inside the kidney's filtering units.
Three large trials drove the shift in practice. The CREDENCE trial, published in the New England Journal of Medicine, found that canagliflozin reduced the risk of kidney failure, doubling of serum creatinine, or death from kidney or cardiovascular causes by about 30 percent in people with type 2 diabetes and albuminuric CKD. The DAPA-CKD trial then showed dapagliflozin slowed CKD progression even in people without diabetes. EMPA-KIDNEY extended the benefit to a broader CKD population, including those with lower albumin levels.
The three SGLT2 inhibitors with the strongest kidney evidence are empagliflozin, dapagliflozin, and canagliflozin. Each is approved for type 2 diabetes, and several are now approved specifically to slow CKD progression regardless of diabetes status. They can be started in many people down to an eGFR of around 20 to 25 mL/min/1.73m², though glucose-lowering effect fades as kidney function declines.
Side effects worth discussing with your doctor include genital yeast infections, mild dehydration, and a small risk of diabetic ketoacidosis. People with frequent urinary tract infections or those on loop diuretics need closer monitoring. Pairing an SGLT2 with a kidney friendly diet for diabetes gives you two levers, medication and food, working in the same direction.
Where SGLT2s Fit in Treatment Order
For someone with type 2 diabetes and CKD, current ADA guidance puts an SGLT2 inhibitor near the top of the list, often alongside metformin, regardless of A1C. That recommendation reflects the kidney and heart benefits, not just the glucose effect. If your doctor has not raised this class with you and you have CKD, it is a reasonable question to ask.
GLP-1 Receptor Agonists: Emerging Kidney Evidence
Glucagon-like peptide-1 (GLP-1) receptor agonists have been mainstays of type 2 diabetes treatment for years, mostly known for blood sugar lowering, weight loss, and cardiovascular protection. The kidney story has caught up. The FLOW trial, published in 2024, was the first dedicated kidney outcomes trial for a GLP-1 agonist and showed that semaglutide reduced the risk of major kidney events by 24 percent compared with placebo in people with type 2 diabetes and CKD.
Common GLP-1 options include semaglutide (weekly injection or oral), liraglutide (daily injection), and dulaglutide (weekly injection). They work by amplifying the body's own insulin response after meals, slowing stomach emptying, and reducing appetite. Most are dosed without major adjustment in mild to moderate CKD, though the National Kidney Foundation advises caution in advanced disease, especially if dehydration from nausea or vomiting is a risk.
Side effects skew toward the gastrointestinal: nausea, occasional vomiting, and reduced appetite, particularly when starting or increasing the dose. Slow titration helps. For people who also have obesity, heart failure, or atherosclerotic cardiovascular disease, the case for a GLP-1 strengthens further. Some people are now on both an SGLT2 inhibitor and a GLP-1 agonist, with each contributing different protective effects.
Metformin: Safe with Adjustments
Metformin remains a first-line diabetes medication for most people with type 2 diabetes, including many with CKD. For decades it was avoided once kidney function dropped because of fear of lactic acidosis, but more recent data led the National Institute of Diabetes and Digestive and Kidney Diseases and the FDA to revise guidance. The eGFR thresholds, not serum creatinine alone, now drive the decision.
Current eGFR-based rules look roughly like this. Above 45 mL/min/1.73m², metformin is generally fine at standard doses. Between 30 and 45, a dose reduction is appropriate, and starting metformin in this range is usually avoided. Below 30, metformin is typically stopped. These thresholds are not absolute, and your clinician may adjust based on the trajectory of your kidney function and other health factors.
Metformin is inexpensive, well-studied, and pairs comfortably with SGLT2 inhibitors and GLP-1 agonists. The most common side effect is gastrointestinal upset, which often improves with extended-release formulations or taking it with food. Keep metformin on the radar at every kidney check-in, since dosing should be revisited any time your eGFR shifts meaningfully. Our breakdown of CKD stages with diabetes shows how those thresholds align with each stage.
Insulin: Always an Option
Insulin works regardless of kidney function, which makes it the dependable backbone when other agents are limited or contraindicated. People with type 1 diabetes have always needed insulin, of course. For people with type 2 diabetes whose kidneys have declined to a point where oral options are narrowing, insulin often steps in.
The wrinkle is that the kidneys clear a meaningful share of injected insulin. As kidney function falls, insulin lingers longer in circulation, which raises the risk of hypoglycemia. That usually means lower total daily doses and closer monitoring, particularly around meals and overnight. People on dialysis sometimes need substantial dose reductions on dialysis days.
Long-acting insulins like glargine and degludec, paired with rapid-acting insulin at meals, are common patterns. A continuous glucose monitor becomes especially helpful here because it surfaces nighttime lows you might otherwise miss. The same flexibility that makes insulin useful in CKD also makes it easier to mismanage, so frequent contact with your diabetes team matters more, not less.
From My Experience
From my experience: I have lived with type 1 diabetes for 14 years and watched friends with type 2 navigate the move from oral medications to insulin as their kidneys changed. The hardest part is rarely the injections, it is the recalibration. Doses that worked perfectly for years suddenly cause lows, and that can shake your confidence. A continuous glucose monitor and a willingness to call your endocrinologist between visits made the biggest difference for the people I know who handled this transition well.
Medications to Use with Caution or Avoid
Not every diabetes medication ages well alongside CKD. A few classes deserve a careful second look as kidney function declines, even when they have served you for years.
Sulfonylureas, including glipizide, glyburide, and glimepiride, increase the risk of prolonged hypoglycemia in CKD because they and their active metabolites are cleared by the kidneys. Glyburide is generally avoided altogether in significant CKD. Glipizide is typically preferred if a sulfonylurea is needed, but most guidelines push for alternatives once kidney function drops.
DPP-4 inhibitors such as sitagliptin, saxagliptin, and alogliptin can be used in CKD, but most need dose reductions as eGFR falls. Linagliptin is the exception and does not require dose adjustment. Alpha-glucosidase inhibitors like acarbose are generally avoided in advanced CKD because of accumulation. Thiazolidinediones such as pioglitazone are not contraindicated by kidney function but can worsen fluid retention, which matters in CKD where edema is already a concern.
Two non-diabetes medication notes deserve mention here. ACE inhibitors and ARBs remain foundational for kidney protection in albuminuric CKD, and finerenone is a newer mineralocorticoid receptor antagonist with kidney and heart benefits in type 2 diabetes with CKD. These are not blood sugar drugs, but they belong in the conversation. For more on the blood pressure side, see our piece on blood pressure medication and diabetes.
The simplest rule we can offer is this. Bring your full medication list, including supplements, to every kidney appointment. Ask whether each item still fits where your eGFR is now, not where it was at diagnosis.
A Practical Next Step
The best diabetes medication for kidney disease is rarely a single drug. It is usually a small, well-chosen combination, often built around metformin if eGFR allows, layered with an SGLT2 inhibitor and possibly a GLP-1 receptor agonist, with insulin reserved for when those options are not enough. The mix evolves with your numbers.
At a glance, here is how the main options compare for someone with type 2 diabetes and CKD:
Before your next appointment, write down your current eGFR, urine albumin-to-creatinine ratio, and A1C. Ask your clinician three questions: which of my medications protects my kidneys, which need a dose change at my current eGFR, and is there a class I should be on that I am not. That single page of notes shapes a far better visit than walking in cold.
Frequently Asked Questions
Which diabetes medications are safest for kidneys?
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) and GLP-1 receptor agonists are the classes with the strongest kidney safety and protective evidence in type 2 diabetes. Metformin is also considered safe with appropriate dose adjustments down to an eGFR of around 30. The right pick depends on your eGFR, albuminuria, and other health conditions, so the choice belongs to a conversation with your provider.
Can diabetes medication help protect the kidneys?
Yes, several can. SGLT2 inhibitors have shown clear kidney protection in trials including CREDENCE, DAPA-CKD, and EMPA-KIDNEY. GLP-1 agonists, particularly semaglutide in the FLOW trial, also reduce major kidney events. These benefits appear to extend beyond what would be expected from blood sugar lowering alone, which is why guidelines now recommend them early for people with type 2 diabetes and CKD.
Does metformin harm the kidneys?
Metformin does not damage the kidneys at appropriate doses. The historical caution was about lactic acidosis when metformin accumulated in advanced kidney disease. Modern guidance allows metformin down to an eGFR of around 30 with dose reduction, and stops it below that. Talk to your doctor about whether your current dose still fits your kidney function.
The honest takeaway here is that the best diabetes medication for kidney disease is usually a layered plan rather than a single pick. SGLT2 inhibitors lead the conversation for most people with type 2 diabetes and CKD, GLP-1 agonists add complementary benefit, metformin still fits at most eGFR levels with the right dose, and insulin remains the dependable option when the others run out of room. Bring your numbers to each visit and let the medication mix evolve with them.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.