What Is Diabetes? The Only Guide You Need
What is diabetes, really? A clear, complete guide to the types, causes, diagnosis, and day-to-day management of every form of diabetes in plain language.

In this article(25)
What is diabetes, really? Beyond the blood sugar numbers and medical jargon, diabetes is a metabolic condition that affects how your body turns food into energy. Whether you are newly diagnosed, supporting someone who is, or just want to understand the basics, this guide covers every type, every cause, and every question in one place.
The word "diabetes" gets used as a single label, but the reality is that several different conditions sit under that umbrella. They share one core feature (elevated blood sugar) but differ in what causes them, how they progress, and how they are treated. Mixing them up is one of the most common sources of confusion for people who are new to the topic.
This guide is meant to be a starting point you can return to. It is long, but each section stands on its own. Skim what you already know, slow down where you have questions, and follow the internal links to deeper coverage when something catches your attention.
What Is Diabetes and How Does It Work
To understand what diabetes is, it helps to understand what is supposed to happen first. According to the American Diabetes Association, diabetes is fundamentally a problem with the way the body uses glucose, the main sugar that fuels every cell.
When you eat, your body breaks carbohydrates down into glucose, which enters the bloodstream. The pancreas, a small organ behind the stomach, releases a hormone called insulin in response. Insulin acts like a key. It opens cells so glucose can move from the blood into them, where it gets used for energy or stored for later.
In someone without diabetes, this system is constant and quiet. Blood sugar stays in a narrow range, around 70 to 140 mg/dL throughout the day, even after meals. Insulin levels rise and fall in step with what you eat, what you do, and what your body needs.
Diabetes happens when this system breaks down in one of two main ways. Either the pancreas does not make enough insulin (insulin deficiency), or the cells of the body stop responding to insulin properly (insulin resistance), or some combination of both. Without enough working insulin, glucose builds up in the blood instead of moving into cells. The cells go hungry. The blood becomes glucose-rich. And every organ in the body, from the eyes to the kidneys to the nerves, has to operate in an environment that is not the one it was designed for.
Why does blood sugar regulation matter so much? Because nearly every system in the body depends on glucose for fuel and on a stable blood environment to function. Persistently high blood sugar damages small blood vessels and nerves over years, which is what drives most long-term diabetes complications. Persistently low blood sugar, on the other hand, can be an immediate emergency because the brain depends on a steady glucose supply.
The simplest way to think about diabetes is as a condition where the body has lost the ability to keep blood sugar in a healthy range on its own. Treatment, in every form of diabetes, is the work of restoring that balance from the outside (with insulin, medication, food choices, movement, and monitoring) until the body is in a stable rhythm again.
Types of Diabetes Explained
Diabetes mellitus is the medical term for the broader condition, and it includes several distinct types. Lumping them together causes more confusion than clarity, especially because treatment looks very different for each. Our piece on diabetes mellitus misconceptions covers the most common mix-ups.
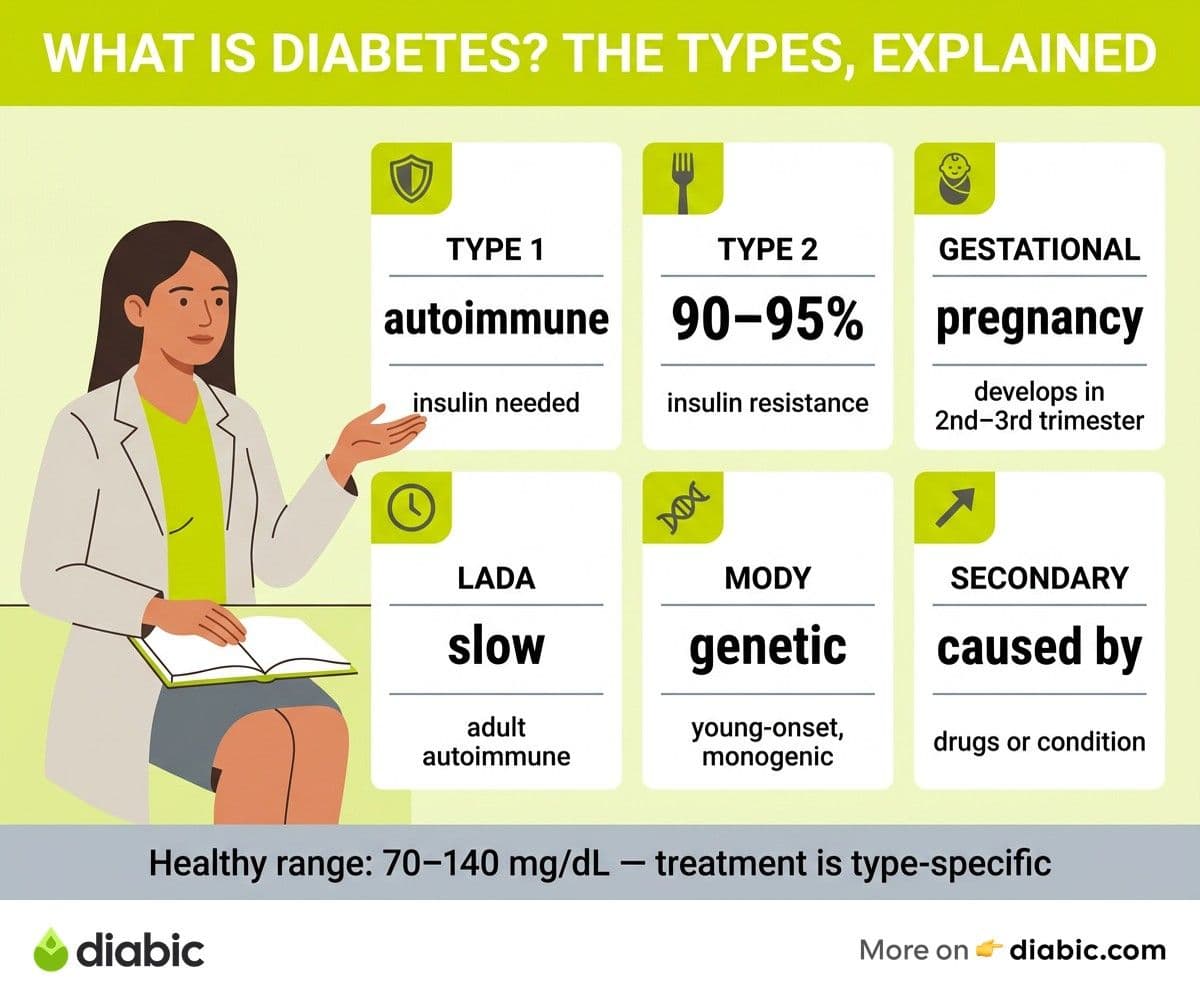
According to the World Health Organization, the major categories are type 1, type 2, gestational, and a handful of less common forms. Each has its own cause, timeline, and management approach.
Type 1 Diabetes
Type 1 diabetes is an autoimmune condition. For reasons researchers are still unraveling, the immune system mistakenly attacks and destroys the insulin-producing beta cells in the pancreas. Once enough beta cells are gone, the body produces little to no insulin of its own.
Type 1 can appear at any age, though it is most often diagnosed in children, teenagers, and young adults. The onset is typically fast, with symptoms developing over days to weeks. Sudden weight loss, intense thirst, frequent urination, and fatigue are the classic cluster. Our deeper explainer on what is type 1 diabetes covers the autoimmune process in more detail.
Treatment is insulin replacement, every day, for life. People with type 1 use a combination of long-acting and rapid-acting insulin, delivered by injection or insulin pump. Continuous glucose monitors (CGMs) have made management easier and safer than it was even a decade ago, but the daily work is still real.
Latent autoimmune diabetes in adults (LADA), sometimes called type 1.5, is a slower form of type 1 that appears in adults and is often initially misdiagnosed as type 2. Autoantibody testing is what distinguishes the two.
Type 2 Diabetes
Type 2 diabetes is the most common form, accounting for roughly 90 to 95 percent of all diabetes cases. It begins with insulin resistance: the cells of the body stop responding well to insulin. The pancreas compensates by producing more, sometimes for years, until it eventually cannot keep up. At that point, blood sugar rises and a diabetes diagnosis follows. Our piece on what is type 2 diabetes walks through the process in plain language.
The onset is gradual. Many people live with elevated blood sugar for years before they are diagnosed, often through routine bloodwork rather than symptoms. When symptoms do appear, they tend to be milder versions of the type 1 cluster: thirst, fatigue, blurred vision, and slow healing.
Treatment varies based on how far the disease has progressed. Lifestyle changes (movement, dietary shifts, sleep, stress management, and weight management when applicable) are the foundation. Medications come in many classes, with metformin most commonly first. Some people eventually need insulin. Many do not. Type 2 management has changed significantly in the past decade as newer medications (GLP-1 receptor agonists, SGLT2 inhibitors) have become more widely available.
Gestational Diabetes
Gestational diabetes is a form of diabetes that develops during pregnancy, usually in the second or third trimester. Pregnancy hormones reduce insulin sensitivity, and most pregnant bodies adapt by producing more insulin. When the pancreas cannot keep up, blood sugar rises.
Gestational diabetes is screened for routinely between 24 and 28 weeks of pregnancy. Treatment focuses on dietary adjustments, monitoring, and sometimes insulin or medication. Most cases resolve after delivery, but a history of gestational diabetes raises long-term risk of type 2, which is why ongoing screening matters even after a healthy delivery.
Prediabetes
Prediabetes is the warning stage before type 2. Blood sugar is higher than normal but not yet in the diabetes range. Specifically, fasting glucose between 100 and 125 mg/dL, A1C between 5.7 and 6.4 percent, or an oral glucose tolerance test reading between 140 and 199 mg/dL. The CDC estimates that more than one in three American adults has prediabetes, and most do not know it.
Prediabetes is the stage where lifestyle changes have the most impact. According to the Diabetes Prevention Program, modest weight loss combined with regular physical activity can reduce progression to type 2 by more than half. Catching it here changes the trajectory of the next 20 years.
Less Common Types
Several other forms of diabetes exist, and while they are less common, they matter for the people they affect.
LADA (latent autoimmune diabetes in adults) was mentioned above. It is essentially slow-onset type 1 in adults.
MODY (maturity-onset diabetes of the young) is a group of inherited forms of diabetes caused by single-gene mutations. It often appears in adolescence or young adulthood and runs strongly in families. MODY can sometimes be managed with oral medications rather than insulin, depending on the specific gene involved.
Neonatal diabetes is rare and appears in babies under six months old. It can be transient or permanent and is genetic in origin.
Secondary diabetes is caused by another medical condition or medication. Diseases of the pancreas (like cystic fibrosis or pancreatitis), hormonal disorders (like Cushing's syndrome or acromegaly), and certain medications (like long-term steroids or some antipsychotics) can all trigger diabetes. Treating or removing the underlying cause sometimes resolves the diabetes; sometimes it does not.
You may also see references to "type 3 diabetes," a term sometimes used to describe a proposed link between insulin resistance and Alzheimer's disease. Our piece on what is type 3 diabetes covers what the research actually says and what the term means.
What Causes Diabetes
The causes of diabetes vary substantially by type. Putting them in one bucket is part of why public understanding is so often off. According to the CDC, the underlying mechanisms differ even though the end result (high blood sugar) looks the same.
Causes of Type 1 Diabetes
Type 1 is autoimmune. The immune system attacks beta cells. Why this happens is not fully understood, but research points to a combination of genetic susceptibility and environmental triggers, possibly including certain viral infections. Type 1 is not caused by lifestyle, diet, or anything a parent or person did or did not do. This matters to say clearly because old myths still linger.
Family history matters but is not destiny. Most people with type 1 do not have a family history. Conversely, having a parent or sibling with type 1 raises risk only modestly compared to the general population. Genetic testing for autoantibodies can identify children at higher risk, and screening programs are expanding for at-risk siblings.
Causes of Type 2 Diabetes
Type 2 has multiple contributing causes. Genetics play a strong role, often stronger than they do in type 1. If a parent or sibling has type 2, your risk is significantly elevated. Body composition (especially visceral fat around the midsection), physical inactivity, sleep quality, chronic stress, and dietary patterns all influence whether and when insulin resistance progresses to diabetes.
It is worth saying clearly that type 2 is not caused by eating too much sugar, and people with type 2 are not at fault for their diagnosis. Genetic predisposition is the foundation, and environment shapes how that predisposition expresses itself. Shame is a poor teacher, and the research is increasingly clear that compassionate, sustainable lifestyle changes outperform restrictive or punishing approaches.
Causes of Gestational Diabetes
Pregnancy hormones reduce insulin sensitivity, particularly in the second and third trimesters. Most pregnant bodies adapt; those with underlying insulin resistance or genetic susceptibility may not. Risk factors include family history, prior gestational diabetes, PCOS, age over 35, and being overweight before pregnancy.
Causes of Less Common Types
LADA shares the autoimmune cause of type 1. MODY is genetic, with specific gene mutations identified for each subtype. Neonatal diabetes is also genetic. Secondary diabetes follows from another condition or medication, as described above.
Why do different types have different causes? Because diabetes is not one disease. It is a family of conditions that all end in elevated blood sugar but begin in different places. Treatment that works for one type can be wrong (sometimes dangerously wrong) for another. This is why correct diagnosis is so important and why broad public messaging that treats all diabetes the same falls short.
How Diabetes Is Diagnosed
Diabetes diagnosis is straightforward in concept and uses a small number of standard tests. According to the NIDDK, any of the following can confirm diabetes when the result is at or above the threshold.
Fasting blood glucose. Measured after at least eight hours without food. A reading of 126 mg/dL or higher on two separate occasions confirms diabetes. Between 100 and 125 mg/dL is prediabetes. Below 100 is normal.
A1C (glycated hemoglobin). This test reflects average blood sugar over the previous two to three months. An A1C of 6.5 percent or higher confirms diabetes. Between 5.7 and 6.4 percent is prediabetes. Below 5.7 is normal. A1C does not require fasting, which makes it convenient.
Oral glucose tolerance test (OGTT). You drink a measured glucose solution and have your blood drawn at intervals over two hours. A two-hour reading of 200 mg/dL or higher confirms diabetes. This test is most often used in pregnancy to screen for gestational diabetes.
Random blood glucose. A reading of 200 mg/dL or higher with classic symptoms (thirst, frequent urination, weight loss) is enough to diagnose diabetes without further testing.
For type 1 specifically, autoantibody tests identify the autoimmune process, and a C-peptide test measures how much insulin the body is producing on its own. Both help distinguish type 1 from type 2 in cases where the diagnosis is unclear, particularly for adults. For a deeper look at one specific type, our piece on what is type 3 diabetes covers how researchers are using diagnostic frameworks beyond the standard categories.
Screening recommendations vary by age and risk factor. The ADA suggests starting routine screening at age 35 for adults with no symptoms or risk factors, and earlier for adults with overweight or obesity plus one or more risk factors (family history, sedentary lifestyle, history of gestational diabetes, PCOS, or certain ethnic backgrounds with elevated risk). Children with overweight and additional risk factors should also be screened.
If you have any classic symptoms of diabetes, do not wait for a routine appointment. Same-week testing through your primary care provider or an urgent care clinic gives you a clear picture and a starting point.
Managing Diabetes Day to Day
Diabetes management is the daily, weekly, and lifelong work of keeping blood sugar in a healthy range while living a full life. The specifics differ by type, but the major levers are similar. According to Mayo Clinic, most management plans share a small set of core elements.
Blood Sugar Monitoring
Knowing your numbers is the foundation. The tools have improved dramatically in the past decade.
Fingerstick meters give a single point-in-time reading and are still widely used. Continuous glucose monitors (CGMs) are small wearable sensors that track blood sugar every few minutes and send data to a phone or receiver. CGMs have transformed type 1 management and are increasingly used in type 2 as well, especially for people on insulin or trying to understand how food and movement affect their blood sugar.
Common targets, from the ADA, are an A1C below 7 percent for most adults (with individualized goals for older adults, children, pregnancy, and other contexts), fasting glucose of 80 to 130 mg/dL, and post-meal glucose under 180 mg/dL one to two hours after eating. Your provider will help set targets that fit your situation.
Insulin Therapy and Oral Medications
People with type 1 use insulin from day one and for life. Most use a basal-bolus approach: a long-acting insulin to cover background needs and a rapid-acting insulin to cover meals and corrections. Insulin pumps and automated insulin delivery systems combine the two and respond to CGM data in real time.
People with type 2 may use a wide range of medications. Metformin is the most common first-line option. Newer classes (GLP-1 receptor agonists like semaglutide, SGLT2 inhibitors like empagliflozin) have become important options because of their additional benefits for weight, cardiovascular health, and kidney function. Some people with type 2 eventually use insulin, often combined with oral medications.
Medication choices are highly individual. Cost, side effects, other health conditions, and personal preferences all shape what fits. This is a conversation to have with your provider, not something to optimize from an article.
Diet and Exercise
There is no single correct diet for diabetes. Mediterranean, lower-carb, plant-forward, and balanced patterns all show benefit in research. The patterns that work best long term tend to share a few features: more vegetables and whole foods, less ultra-processed food and added sugar, adequate protein, and sustainable enjoyment.
Carbohydrate awareness matters more for some people than others. People on insulin generally need to count or estimate carbs to dose accurately. People on metformin or lifestyle alone may benefit from understanding carb timing and quality without precise counting. The right level of detail depends on what is helping your blood sugar and what is helping you live well.
Exercise is one of the most powerful tools available. Regular movement improves insulin sensitivity, lowers post-meal blood sugar, supports heart health, and helps with mood and sleep. Combining cardio (walking, cycling, swimming) with resistance training (weights, bands, bodyweight) is the pattern most consistently associated with metabolic improvements. Consistency matters more than intensity.
Building a Care Team
Diabetes management works best as a team effort. The team typically includes a primary care doctor or endocrinologist, a certified diabetes care and education specialist (CDCES), a registered dietitian, an eye doctor for annual exams, a podiatrist for foot care, and sometimes a mental health professional. Mental and emotional support matter; diabetes burnout is real and common.
Community matters too. Peer support, whether through online groups, local meetups, or apps like ours, helps with the parts of diabetes that medicine alone cannot address. Living with a chronic condition is easier when you are not doing it alone.
Living Well With Diabetes
Diabetes management is about numbers, but living well with diabetes is about much more than that.
Mental Health and Diabetes Burnout
People with diabetes are at higher risk for depression, anxiety, and a specific phenomenon called diabetes burnout. Burnout shows up as exhaustion with the daily demands, frustration with numbers that will not cooperate, withdrawal from self-care, and a sense of failure that does not match the actual effort being put in.
Burnout is not a moral failing. It is a predictable response to a condition that asks for attention every few hours, every day, with no days off. Recognizing it early matters because untreated burnout often leads to worsening blood sugar, missed medications, and a downward spiral. Therapy with someone who understands chronic illness, peer support, and structured breaks (like temporarily simplifying targets) all help. Talk to your doctor if you think you may be in burnout.
Community Support and Peer Connections
Diabetes is one of the most studied chronic conditions in the world, and one of the loneliest to live with. Peer connections, whether online or in person, are not optional extras. They are part of how people sustain self-care over years and decades.
Hearing someone else describe the exact thing you have been struggling with (a stubborn dawn phenomenon, a frustrating CGM sensor, the awkwardness of dosing for a wedding cake) is genuinely therapeutic. It also makes practical knowledge transfer faster than any textbook.
Technology That Makes Management Easier
The technology landscape has changed faster in the past decade than in the previous fifty years combined. CGMs, insulin pumps, automated insulin delivery (AID) systems, smart pens, food and activity tracking apps, and decision-support tools have all made daily management more precise and less exhausting.
Not every tool fits every person. Some people thrive with a CGM and a pump; others prefer a meter and pens. The technology that fits is the one you will actually use and that improves both your numbers and your quality of life. Your care team can help you sort through the options.
For a deeper look at how the major types compare side by side, our piece on type 1 vs type 2 differences covers the practical contrasts in daily life, treatment, and long-term planning.
From my experience: I have lived with type 1 diabetes for 14 years. The single biggest shift in how well I have lived with it was not a new technology or a perfect diet. It was finding people who actually got it. The first time someone in a peer group casually mentioned the same exact frustration I had been carrying alone for two years, something inside me unclenched. The numbers got easier after that, partly because the rest of life got lighter. Whatever your type, find your people. The technical side of diabetes responds to medicine. The human side responds to community.
FAQ
What are the different types of diabetes?
The main types are type 1 (autoimmune), type 2 (insulin resistance, often combined with declining insulin production), gestational (during pregnancy), and prediabetes (elevated blood sugar that is not yet at the diabetes threshold). Less common types include LADA (latent autoimmune diabetes in adults), MODY (maturity-onset diabetes of the young), neonatal diabetes, and secondary diabetes caused by other medical conditions or medications. Each type has different causes, progression, and treatment approaches, which is why correct identification matters for choosing the right care plan.
What causes diabetes and how is it managed?
Diabetes causes vary by type. Type 1 is caused by an autoimmune attack on insulin-producing beta cells in the pancreas. Type 2 results from insulin resistance compounded by genetics, body composition, sleep, stress, and lifestyle factors. Gestational diabetes follows from pregnancy hormones reducing insulin sensitivity in someone whose pancreas cannot keep up. Management depends on the type but generally includes blood sugar monitoring, insulin therapy or oral medications, dietary patterns that support steady blood sugar, regular physical activity, and consistent follow-up with a healthcare team. Diabetes management is a long-term practice, and there is meaningful room to live well at every stage.
If you came to this page asking what is diabetes and what to do next, the short answer is that you are looking at a family of conditions, all centered on blood sugar regulation, all manageable with the right combination of information, medication, and habits. Bookmark the type that fits your situation, follow the deeper guides linked above, and treat this page as a map you can keep returning to as your questions evolve.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Diabetes Knowledge
View all
Small Lifestyle Changes for Prediabetes, Big Results
A small lifestyle change for prediabetes, done consistently, can rival medication. Here is what actually works and how to build habits that stick.

Low Blood Sugar Symptoms That Hit Without Warning
Learn the low blood sugar symptoms that strike without warning, how to respond fast with the ADA Rule of 15, and when to call for help.

Weight Loss for Prediabetes: A Realistic Approach
Weight loss for prediabetes does not require extreme dieting. Learn the 5-7% target, what works, and how to set realistic, sustainable goals.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.