Prediabetes: Why Catching It Now Changes Everything
Prediabetes affects 98 million US adults and most do not know. Catching it early opens a window where small actions can prevent type 2 diabetes.

In this article(14)
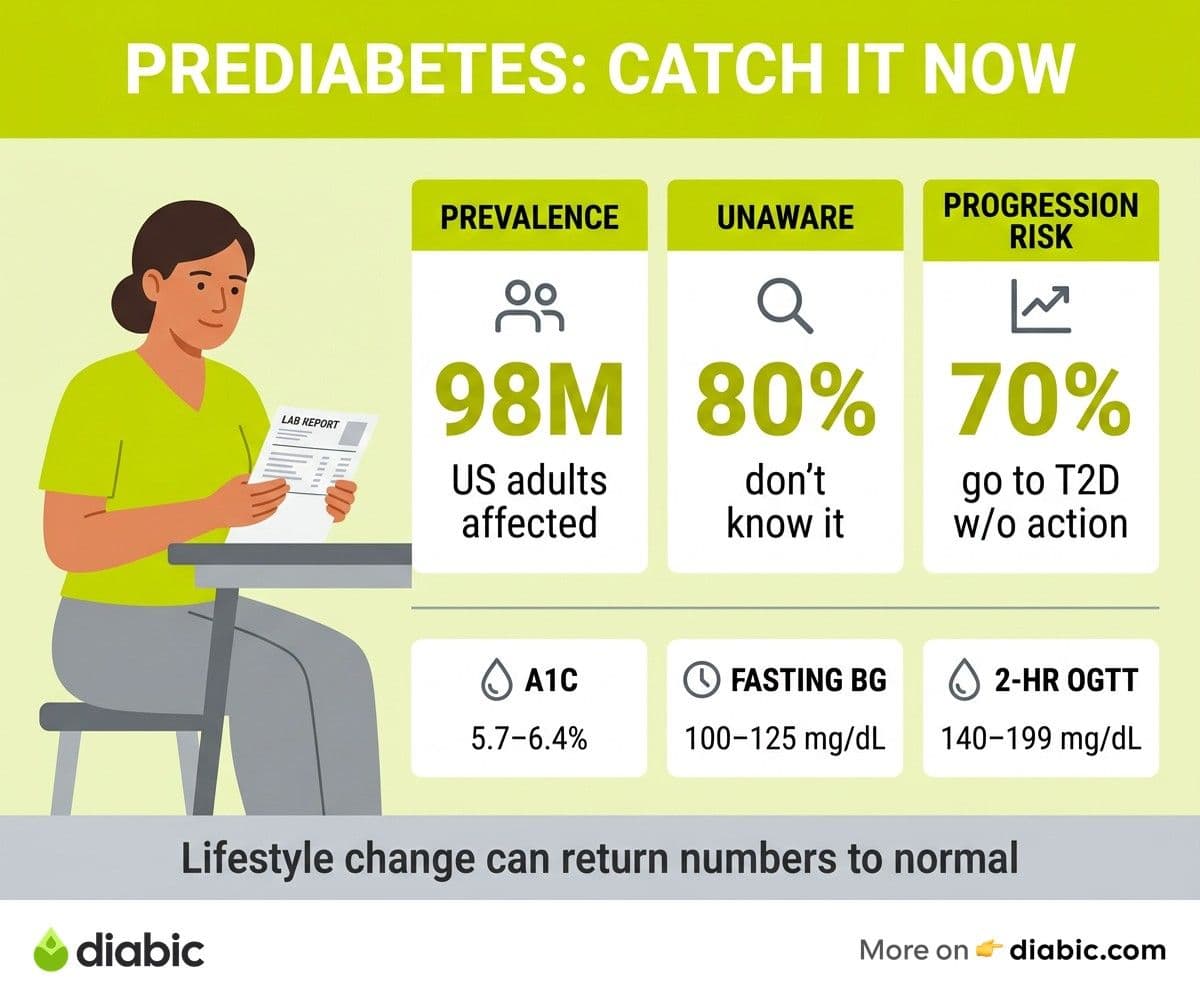
Prediabetes affects an estimated 98 million American adults, and roughly 80 percent of them have no idea. The condition rarely causes obvious symptoms, blood tests catch it only when someone thinks to order them, and the warning signs are easy to mistake for ordinary tiredness or stress.
That quiet quality is also what makes this stage such an opportunity. Caught now, before it crosses into type 2 diabetes, it sits in a window where moderate lifestyle changes can change your trajectory by decades. This is where small actions still produce the biggest results, and the choice you make now is genuinely different from the choice you would face after a type 2 diagnosis.
What Prediabetes Is and Why It Matters
Prediabetes means your blood sugar is higher than normal but not yet high enough to be classified as type 2 diabetes. Specifically, the CDC defines it as an A1C between 5.7 and 6.4 percent, a fasting blood glucose between 100 and 125 mg/dL, or a two-hour glucose tolerance result between 140 and 199 mg/dL.
These are not arbitrary cutoffs. They mark the range where insulin resistance is already established, the pancreas is already working overtime, and the long-term risks of type 2 diabetes start climbing measurably. Without intervention, research suggests that up to 70 percent of people with prediabetes go on to develop type 2 diabetes during their lifetime.
That number is sobering, but it is not a sentence. The same research that produced the 70 percent figure also showed that the progression is preventable in most cases. The body responds to even modest changes in diet, movement, and weight, and the response is faster at the prediabetes stage than after years of full diabetes have set in.
The framing matters more than the numbers. Prediabetes is not a softer version of diabetes. It is a separate, reversible window that closes a little more each year it goes unaddressed.
What Is Prediabetes Doing to Your Body
By the time blood sugar enters this borderline range, insulin resistance is already in motion. The cells in your muscles, fat, and liver have become less responsive to insulin's signal to absorb glucose, and the pancreas compensates by producing more insulin to keep blood sugar in check. The NIDDK explains this compensation as the early phase of what eventually becomes type 2 diabetes if the pancreas can no longer keep up.
That extra insulin is not benign. Higher circulating insulin is associated with weight gain around the midsection, higher blood pressure, and unfavorable cholesterol patterns. The combination is sometimes called metabolic syndrome, and it sets up risk well beyond blood sugar itself.
Quiet damage may also begin during this stage. Some studies have found early signs of nerve and blood vessel changes in people with elevated but not yet diabetic glucose, including a small but measurable increase in cardiovascular risk. The damage is not the dramatic kind that produces symptoms. It is the slow kind that builds up over years.
This is also why most people feel completely fine despite elevated blood sugar. The body is still managing, just barely, and the margin between "managing" and "not managing" is narrower than it feels. For a closer look at what does eventually show up, our coverage of prediabetes symptoms walks through the subtle changes that sometimes appear.
How Prediabetes Is Diagnosed
Prediabetes is diagnosed by blood test, not by symptoms. The American Diabetes Association recognizes three tests, any of which can confirm the condition.
The fasting blood glucose test measures blood sugar after at least eight hours without food. A result between 100 and 125 mg/dL falls in the prediabetes range. Above 126 mg/dL on two occasions confirms diabetes.
The A1C test reflects average blood sugar over the previous two to three months by measuring the percentage of glycated hemoglobin. A result of 5.7 to 6.4 percent indicates prediabetes. The A1C is convenient because it does not require fasting and gives a longer view than a single snapshot.
The oral glucose tolerance test (OGTT) measures blood sugar two hours after drinking a standardized glucose solution. A result of 140 to 199 mg/dL indicates prediabetes. The OGTT is sensitive but more time-consuming, so it is more commonly used in pregnancy or when other tests are inconclusive.
Routine screening catches what symptoms cannot. The ADA now recommends screening starting at age 35 for all adults, and earlier for those with risk factors like overweight, family history, or a history of gestational diabetes. If you have not been tested in the last three years, asking your doctor at your next visit takes only a minute.
If you have already received an A1C result and want to understand what the number actually means in context, our explainer on prediabetes A1C meaning covers the ranges and what they suggest about progression.
What Is Pre Diabetes Telling You About the Future
A pre diabetes diagnosis is essentially a 10-year forecast of where things are heading without intervention. Most people with this condition will develop type 2 diabetes within 10 to 20 years if nothing changes, and many cardiovascular risks begin accumulating during the early window itself.
That is the part most people miss. The risks of type 2 diabetes do not arrive with the diagnosis. They build during the years before, which means the earlier you act, the more risk you can erase before it materializes.
The good news baked into that forecast is that the trajectory can be redirected. Not just slowed, but in many cases reversed back to normal blood sugar. The next sections cover what makes that redirection possible.
Who Is at Risk for Prediabetes
The condition does not discriminate, but some factors raise the odds significantly. The clearest risk factors include:
- Being overweight or having a higher waist circumference
- Being aged 45 or older, with risk climbing further after 65
- Having a parent or sibling with type 2 diabetes
- A history of gestational diabetes or giving birth to a baby weighing more than 9 pounds
- Being of African American, Hispanic or Latino, Native American, Asian American, or Pacific Islander heritage
- A sedentary lifestyle, defined as less than 150 minutes per week of moderate activity
- Polycystic ovary syndrome (PCOS), high blood pressure, or unfavorable cholesterol numbers
- Sleep disorders, including obstructive sleep apnea
The Mayo Clinic's overview of prediabetes lists these factors and emphasizes that having one or more does not guarantee a diagnosis. It does, however, mean a baseline screening is worth requesting.
Risk profiles can also stack. Someone with a family history, midlife age, and a desk job carries meaningfully more risk than any one of those factors alone. Knowing your stack helps you push for testing without having to wait for symptoms that may never come.
What You Can Do Right Now
The most studied intervention at this stage is the Diabetes Prevention Program, a structured lifestyle change protocol developed in a landmark NIH-funded trial. The program asks for two specific things: 7 percent body weight loss and 150 minutes of moderate physical activity per week. Participants who reached those targets cut their risk of type 2 diabetes by 58 percent.
Translated into daily life, that looks like:
- Dietary changes. Reducing refined carbohydrates and sugary drinks, and adding more fiber from vegetables, beans, fruit, and whole grains. Lean protein at most meals helps with satiety and blood sugar both. Our prediabetes diet guide breaks the patterns down in detail.
- Physical activity. Thirty minutes of brisk walking, five days a week, hits the 150-minute target. Anything that gets your heart rate up counts, including cycling, swimming, dancing, or yard work. Reducing long sitting blocks helps too.
- Weight loss. For someone weighing 200 pounds, the 7 percent target is about 14 pounds. Even 5 percent produces measurable benefit. Slow, steady loss tends to stick longer than rapid loss.
These three threads reinforce one another. Movement makes weight loss easier and improves insulin sensitivity directly. Better food choices make movement feel less like a chore. Modest weight loss makes both feel more sustainable.
Medication is sometimes added to lifestyle changes, particularly for people at very high risk. Metformin is the most commonly considered option at this stage, and the DPP showed it reduced diabetes risk by 31 percent on its own, less than lifestyle but still meaningful. For more on what is available and how decisions are made, see our overview of prediabetes treatment options.
The Good News: Prediabetes Is Reversible
The single most important fact about prediabetes is that it can be reversed. Long-term follow-up of the DPP showed that lifestyle intervention reduced type 2 diabetes incidence by 58 percent over three years, and for participants over 60, the reduction was 71 percent. Twenty-year follow-ups confirmed that the benefit persisted decades later.
For many participants, blood sugar did not just stop progressing. It returned to the normal range. That is what reversal means in this context: A1C and fasting glucose dropping back below the prediabetes thresholds and staying there.
The window matters enormously. Once type 2 diabetes is established, the pancreas has already lost some of its insulin-producing capacity, and recovery becomes harder. During prediabetes, the pancreas is strained but not yet failing, which is why interventions work so reliably here.
For a deeper look at what reversal actually involves and how to know if you are on track, our piece on whether prediabetes can be reversed walks through the evidence and what realistic timelines look like.
From my experience: 14 years into managing diabetes, the conversation I find myself having most often with newly diagnosed friends is not about insulin or carb counting. It is about the years they were prediabetic and did not know it. Almost everyone wishes they had asked for the test earlier. The blood test costs almost nothing, the result either reassures you or hands you an early warning, and that early warning is one of the few moments in adult health where the right action genuinely changes the path.
How to Talk to Your Doctor About Prediabetes
If prediabetes runs in your family, or if you have been told your fasting glucose is in the upper end of normal, asking for an A1C at your next visit is reasonable. The conversation does not need to be complicated. A few useful questions:
- What was my most recent A1C and fasting glucose?
- Given my history, should I be screened more often than every three years?
- If I am in the prediabetes range, what local lifestyle programs do you recommend?
- Would you consider referring me to a registered dietitian or a CDC-recognized National Diabetes Prevention Program?
Recognized prevention programs are often covered by insurance, including Medicare, and they provide structured group support that closely matches the original DPP trial. Asking about them by name often opens doors that "general advice" does not.
The point of the conversation is to convert a quiet number into a clear plan. You do not need to commit to anything dramatic in the appointment itself. You just need to know your number and your options.
FAQ
What does it mean to have prediabetes?
Having prediabetes means your blood sugar is higher than normal but not yet high enough to be classified as type 2 diabetes. It indicates that your body is becoming resistant to insulin and that your pancreas is working harder than it should to maintain blood sugar. It is also an opportunity, since lifestyle changes at this stage can often prevent or significantly delay the onset of type 2 diabetes.
Can prediabetes be stopped from becoming diabetes?
Yes. Research from the Diabetes Prevention Program showed that moderate lifestyle changes, specifically losing 5 to 7 percent of body weight and exercising 150 minutes per week, reduced the risk of developing type 2 diabetes by 58 percent. For people over 60, the reduction was 71 percent. Prediabetes is the stage where intervention is most effective.
What is the meaning of prediabetes on a blood test result?
What is the meaning of prediabetes in a clinical sense comes down to specific lab ranges: an A1C of 5.7 to 6.4 percent, a fasting glucose of 100 to 125 mg/dL, or a two-hour glucose tolerance result of 140 to 199 mg/dL. Any one of those three results, confirmed by your doctor, qualifies as prediabetes.
How long does it take to reverse prediabetes?
Many people see meaningful improvement in fasting glucose within a few weeks of consistent changes, and A1C usually shifts within 8 to 12 weeks. Returning fully to the normal range can take three to six months or longer, depending on starting point and consistency. Talk to your doctor about retesting timelines that make sense for your situation.
Is prediabetes the same as type 2 diabetes?
No. Prediabetes is a separate stage with its own diagnostic ranges and its own window for intervention. The risks overlap, but the choices available to you in prediabetes, particularly the chance to return to normal blood sugar, are not the same as those available after a type 2 diabetes diagnosis.
The most powerful thing about a prediabetes diagnosis is also the most easily missed: it is the moment when your future is still genuinely undecided. Knowing your number, asking your doctor for the next step, and starting with one small change is enough to begin tilting the odds back in your favor.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Diabetes Knowledge
View all
Small Lifestyle Changes for Prediabetes, Big Results
A small lifestyle change for prediabetes, done consistently, can rival medication. Here is what actually works and how to build habits that stick.

Low Blood Sugar Symptoms That Hit Without Warning
Learn the low blood sugar symptoms that strike without warning, how to respond fast with the ADA Rule of 15, and when to call for help.

Weight Loss for Prediabetes: A Realistic Approach
Weight loss for prediabetes does not require extreme dieting. Learn the 5-7% target, what works, and how to set realistic, sustainable goals.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.