Thyrotoxicosis Symptoms and Diabetes: What to Know
Learn how thyrotoxicosis symptoms affect blood sugar in diabetes, why insulin needs change, and the warning signs that mean you should call your doctor.

A racing heart while sitting still. Pounds dropping off the scale even as you eat more. Glucose readings that swing higher than they have in years, despite no change in food, stress, or sleep. When you live with diabetes, these shifts can feel like your management plan suddenly stopped working, when in reality the trigger may be your thyroid.
Thyrotoxicosis symptoms can be unsettling on their own, and when diabetes is part of the picture, the combination can quickly destabilize blood sugar. Recognizing the early signs helps you respond faster, get the right tests, and work with your healthcare team before things escalate. This guide walks through how excess thyroid hormone behaves in the body, what to look for, and why treatment of the thyroid often restores the diabetes balance you had before.
A quick note before we go further. Thyrotoxicosis means your tissues are exposed to too much thyroid hormone, from any cause, and severe thyrotoxicosis (sometimes called thyroid storm) is a medical emergency. Hyperthyroidism, by contrast, is the chronic state of an overactive thyroid gland and is the most common cause of thyrotoxicosis. The two terms are related, but the distinction matters when symptoms turn severe.
Common Thyrotoxicosis Symptoms
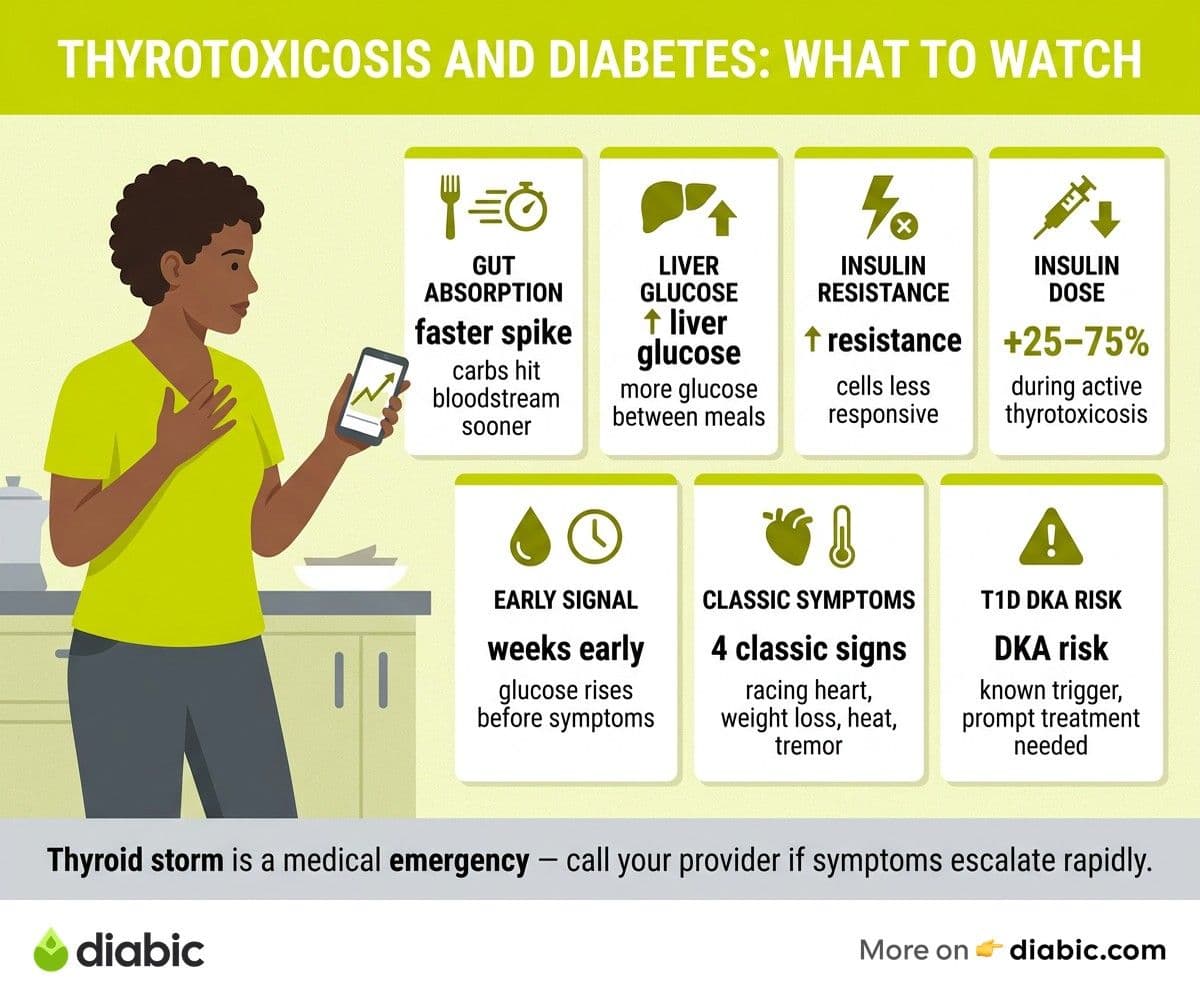
Thyrotoxicosis symptoms tend to mirror a body stuck in fast-forward. Metabolism speeds up, the cardiovascular system works harder, and many of the systems your diabetes plan depends on become harder to predict. According to the American Thyroid Association, the most reported signs include rapid heartbeat, weight loss, anxiety, heat intolerance, and tremor.
Each symptom can show up on its own or in clusters. Some people notice the cardiac changes first. Others register the emotional shifts before anything physical, and a few only realize something is wrong when their blood sugar starts behaving strangely.
Here is what to watch for:
- Rapid heartbeat and palpitations. A resting pulse above 100 beats per minute, fluttering sensations, or new awareness of your own heartbeat at rest.
- Unexplained weight loss despite normal or increased eating. Five to ten pounds in a few weeks is common, even when appetite has gone up.
- Anxiety, tremors, and restlessness. A fine tremor in the hands, racing thoughts, or trouble sitting still during quiet moments.
- Heat intolerance and excessive sweating. Feeling warm in rooms others find comfortable, or sweating through clothes without much exertion.
- Fatigue and muscle weakness. Stairs feel harder, grocery bags feel heavier, and recovery from light exercise takes longer.
- Changes in bowel habits. More frequent stools or mild diarrhea, since gut motility increases with excess thyroid hormone.
If several of these appear together over a few weeks, that pattern deserves a conversation with your provider. Single symptoms in isolation are usually less concerning, but the combination is the red flag.
How These Symptoms Affect Blood Sugar
This is the part that surprises many people with diabetes. The same hormone surge that makes your heart race also rewires how your body handles glucose, often raising blood sugar before any classic thyroid symptom feels obvious. Research published in Endocrine Reviews describes several overlapping mechanisms that drive this effect.
Accelerated glucose absorption from the gut
Excess thyroid hormone speeds up how quickly carbohydrates move through the small intestine and into the bloodstream. A meal that used to peak at 160 mg/dL might now spike to 220 mg/dL with the same plate of food. The post-meal curve also rises faster, which can outpace short-acting insulin that worked fine a month ago.
Increased hepatic glucose production
The liver releases more glucose between meals and overnight, even when insulin levels are adequate. Many people with type 2 diabetes notice fasting numbers creeping up first, while those on insulin may see overnight readings drift higher despite stable basal doses.
Greater insulin resistance and higher insulin requirements
Cells become less responsive to insulin during thyrotoxicosis, so the same dose covers fewer carbs than before. People who use insulin often need temporary increases of 25 to 75 percent during active thyrotoxicosis, with adjustments tapering back as the thyroid is treated. People on oral medication may find their A1C climbing despite no other lifestyle changes.
Why blood sugar often becomes erratic before other symptoms
The metabolic changes can outpace the physical ones. You may see rising glucose, more variability, and unusual lows from over-correction weeks before weight loss or palpitations become obvious. If you track how thyroid affects blood sugar and notice a pattern of rising readings without an obvious cause, it is reasonable to ask about thyroid testing.
Can Thyrotoxicosis Make Diabetes Harder to Manage
Yes, and the impact can be significant. The combination of metabolic overdrive plus existing diabetes creates compounding effects that can shift management quickly.
The compounding effect of metabolic overdrive
Thyrotoxicosis raises both glucose production and insulin resistance, while diabetes already involves either insufficient insulin or impaired insulin response. Stacked together, these shifts mean small carbohydrate intake can produce larger spikes, and the usual correction strategies may not work as expected. Sleep can suffer too, which adds another layer of glucose variability.
Increased risk of diabetic ketoacidosis in type 1 diabetes
This is the safety issue that needs the most attention. A study in Diabetes Care found that thyrotoxicosis can precipitate diabetic ketoacidosis (DKA) in people with type 1 diabetes, sometimes as the first presentation of an undiagnosed thyroid condition. Higher insulin needs, increased lipolysis, and dehydration from heat intolerance and faster gut transit all push in the same direction.
If you have type 1 diabetes and notice persistent high glucose alongside thyrotoxicosis symptoms, check ketones and contact your provider. Do not wait for symptoms to "settle down" on their own.
Why insulin doses may need temporary increases
During active thyrotoxicosis, your endocrine team may walk you through carefully raising basal and bolus insulin to match the new demand. Once antithyroid medication, radioactive iodine, or other treatment brings hormone levels back toward normal, insulin needs typically fall again. This is why frequent contact with your care team during this period helps you avoid both highs from undertreatment and lows from delayed adjustments.
How treatment of thyrotoxicosis stabilizes diabetes management
Most people with diabetes find that as thyroid hormone levels normalize, glucose patterns return closer to their previous baseline within four to twelve weeks. The thyroid treatment is doing the heavy lifting here, and your diabetes plan often needs to step down in parallel. Track your numbers carefully during this taper to catch unexpected lows early.
From my experience: In my fourteen years with type 1 diabetes, I have had two periods where my insulin needs climbed without explanation. The first time I assumed it was stress and burned through three months of frustration before someone ordered a TSH. The second time, I recognized the pattern faster, asked for thyroid labs at my next appointment, and we caught a thyroid flare early. The lesson I keep coming back to: when your usual diabetes math stops working, your thyroid is worth a quick check before you redesign your entire plan.
Hyperthyroidism Symptoms in People with Diabetes
Hyperthyroidism symptoms and the symptoms of poorly managed diabetes can look almost identical from the outside, which is part of why thyroid problems often go undiagnosed for months in people with diabetes. Both conditions can produce fatigue, weight loss, increased thirst, more frequent urination, and irritability.
How symptoms overlap with poorly managed diabetes
Weight loss is the classic example. In type 1 diabetes, weight loss can signal insufficient insulin. In hyperthyroidism, it can signal excess thyroid hormone. The two can coexist, and treating only the diabetes side will not resolve the thyroid driver. Increased appetite paired with weight loss is a particularly strong hint that something beyond diabetes alone is at work.
The challenge of distinguishing thyroid symptoms from diabetes symptoms
A few clues help separate them. A resting heart rate above 100 that does not respond to better glucose levels suggests thyroid involvement. Heat intolerance, hand tremor, and bowel changes lean thyroid as well, since these are uncommon as a result of diabetes alone. Many people with type 1 diabetes also develop autoimmune thyroid conditions, so Graves disease symptoms with diabetes deserve a separate read if your provider mentions Graves as a possibility.
When to suspect hyperthyroidism as the cause of blood sugar problems
Consider asking for thyroid testing when:
- Insulin needs rise more than 20 percent without dietary or activity changes
- A1C climbs unexpectedly while your habits stay consistent
- You feel hot, anxious, or shaky in ways that do not match your glucose readings
- Resting heart rate stays elevated even when blood sugar is in target range
These patterns do not confirm hyperthyroidism, but they are reasonable triggers for a TSH and free T4 test.
Overactive Thyroid Symptoms and Warning Signs
Overactive thyroid symptoms exist on a spectrum, from subtle to severe. Catching the early ones means easier treatment and faster diabetes stabilization. Missing the severe ones can be dangerous.
Early warning signs that are easy to miss
Subtle changes often come first: a slightly faster pulse, mild trouble sleeping, hands that feel a touch shaky during fine tasks, or warm skin you start to notice when others feel cool. People with diabetes sometimes attribute these to caffeine, stress, or low blood sugar. If they persist for more than two or three weeks, they are worth flagging.
When symptom severity warrants urgent medical attention
Call your provider promptly if you have:
- A persistent resting heart rate above 110 beats per minute
- Chest pain or new shortness of breath
- New irregular heartbeats or significant palpitations
- Persistent vomiting that interferes with hydration
- Confusion, agitation, or unusual mental fog
These can signal severe thyrotoxicosis or thyroid storm, especially when paired with high fever or extreme weakness.
Thyroid storm: the rare but serious emergency
Thyroid storm is rare but life-threatening. It involves fever above 101 degrees Fahrenheit, severe tachycardia, gastrointestinal symptoms, and altered mental status. The National Institutes of Health describes thyroid storm as a medical emergency requiring hospital evaluation. If you suspect it, go to the emergency room. Do not try to manage it at home. People with diabetes face an additional risk because thyroid storm can also trigger DKA, which compounds the danger.
Thyroid and Blood Sugar: Getting Tested
If anything in this guide describes what you are experiencing, the next step is straightforward: get tested. Thyroid evaluation is simple, inexpensive, and widely available.
When to request thyroid function tests
The Mayo Clinic recommends thyroid testing whenever symptoms suggest an overactive or underactive thyroid, and the American Diabetes Association Standards of Care recommend routine TSH screening for people with type 1 diabetes given the higher autoimmune overlap. For people with type 2 diabetes, testing is appropriate any time symptoms or unexplained glucose patterns appear.
How TSH, free T4, and T3 help diagnose thyrotoxicosis
The standard panel includes:
- TSH (thyroid-stimulating hormone). Usually low or undetectable in thyrotoxicosis, since the pituitary stops producing TSH when thyroid hormone is high.
- Free T4 and free T3. Typically elevated, confirming the excess hormone state.
- Thyroid antibodies. Useful to identify Graves disease or autoimmune thyroiditis as the underlying cause.
If you want a deeper dive into what a TSH test means for diabetes care, that explainer covers reference ranges and how often to retest.
Working with your endocrinologist on treatment
Treatment options for thyrotoxicosis include antithyroid medications, radioactive iodine, beta-blockers for symptom relief, and in some cases surgery. Each option has different implications for diabetes management, so an endocrinologist who treats both conditions is a strong advantage. Talk to your doctor about how each treatment may affect your insulin or oral medication needs, and what monitoring schedule makes sense as your thyroid hormone levels stabilize.
Frequently Asked Questions
How does an overactive thyroid affect blood sugar?
Excess thyroid hormone speeds up metabolism, increasing glucose production in the liver and accelerating carbohydrate absorption. This raises blood sugar levels and increases insulin requirements, making diabetes harder to manage until the thyroid condition is treated.
Can thyrotoxicosis make diabetes harder to manage?
Yes. Thyrotoxicosis causes insulin resistance and metabolic overdrive that make blood sugar levels erratic and harder to predict. Treatment of the thyroid condition typically restores more stable blood sugar management within several weeks.
Is thyrotoxicosis the same as hyperthyroidism?
Not quite. Hyperthyroidism describes a chronically overactive thyroid gland producing too much hormone. Thyrotoxicosis describes the state of having too much thyroid hormone in the body from any cause, including hyperthyroidism, thyroiditis, or excess medication. Severe thyrotoxicosis (thyroid storm) is a medical emergency.
How long does it take for blood sugar to stabilize after thyroid treatment?
Most people see meaningful improvement within four to twelve weeks of starting treatment. Insulin doses typically need to come back down during this period, so frequent monitoring helps avoid hypoglycemia as your thyroid hormone levels normalize.
Should I see an endocrinologist for both diabetes and thyroid issues?
When both conditions are active, an endocrinologist who manages diabetes and thyroid care together can simplify your plan and improve outcomes. Ask your primary care provider for a referral if you do not already have one.
Where to Go from Here
If your thyrotoxicosis symptoms have been hiding behind unexpected glucose changes, you now have a clearer map of what is happening and what to ask for. Track your blood sugar, note any symptom patterns, and bring both to your next appointment so your team can decide whether thyroid testing is the right next step. Catching it early is the difference between a few weeks of adjustment and months of frustration.
For more on how the thyroid and metabolic system interact, our cluster on thyroid and diabetes covers Graves disease, Hashimoto's, hypothyroidism, and the lab tests that tie them together. Small steps, taken early, protect both your thyroid and your diabetes management plan.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.