Type 1 vs Type 2 Diabetes: How Lab Tests Tell Them Apart
Type 1 vs type 2 diabetes look similar on paper, but lab tests reveal what is really happening. See how A1C, antibodies, and C-peptide guide diagnosis.

In this article(10)
When a new diagnosis lands in your lap, the first question is rarely about treatment. It is usually some version of, "Wait, which kind do I have?" The shorthand label of diabetes hides a fork in the road, and the path through type 1 vs type 2 diabetes runs through the lab, not the symptom list. Two people can walk in with the same thirst, the same fatigue, and the same fasting glucose number, and still leave with very different diagnoses.
We hear from readers all the time who were told "you have diabetes" without a clear explanation of which type, what tests confirmed it, or whether more testing was needed. Type 1 and type 2 share a name and some early symptoms, but the underlying biology is different, and the lab tests that distinguish them shape every decision that follows. This guide focuses on what those tests measure, when each one is ordered, and how to read the results with your provider.
From my experience: When I was diagnosed in my early twenties, I left the ER knowing my A1C number but not whether anyone had ordered antibodies or C-peptide. It took a follow-up visit a few weeks later, and a specific request, before GAD antibodies were drawn and the type 1 picture was confirmed in writing. I tell newly diagnosed friends to ask for copies of every lab from that first month, because those results become the baseline you compare everything else against for years.
How Type 1 vs Type 2 Diabetes Are Diagnosed Initially
The first round of testing for both type 1 vs type 2 diabetes uses the same four diagnostic tools. According to the ADA Standards of Care published in Diabetes Care, diagnosis can be confirmed by any of the following: an A1C of 6.5 percent or higher, a fasting plasma glucose of 126 mg/dL or higher, a 2-hour value of 200 mg/dL or higher on an oral glucose tolerance test, or a random plasma glucose of 200 mg/dL or higher in someone with classic symptoms.
These tests confirm that diabetes exists, but they do not tell your provider which type you have. That gap often surprises newly diagnosed adults. A high A1C looks the same whether the underlying cause is autoimmune destruction of beta cells or insulin resistance built up over years. Distinguishing between the two usually requires a second tier of testing or careful clinical judgment based on age, body composition, and how quickly symptoms appeared.
Type 1 is sometimes diagnosed in an emergency room rather than a primary care office. Severe symptoms, vomiting, or diabetic ketoacidosis (DKA) can lead to rapid testing and an immediate insulin start. Type 2, by contrast, is often picked up on a routine A1C test years after blood sugar started drifting upward. If you are recognizing some of the early signs you might have diabetes, the diagnostic process described here is the next step.
The Core Diagnostic Tests Explained
Each of the four standard tests measures something slightly different. Reading a lab report becomes much less intimidating once you know what each number is actually capturing about your metabolism.
- A1C (glycated hemoglobin): Reflects average blood glucose over the previous 2 to 3 months. Diagnostic at 6.5 percent or higher. Useful because it does not require fasting and is less affected by short-term fluctuations.
- Fasting plasma glucose (FPG): A single point-in-time measurement after at least 8 hours without eating. Diagnostic at 126 mg/dL or higher. Sensitive to recent food, illness, and stress.
- Oral glucose tolerance test (OGTT): Measures blood sugar 2 hours after drinking a standardized 75-gram glucose solution. Diagnostic at 200 mg/dL or higher. Often used in pregnancy and when other tests are inconclusive.
- Random plasma glucose: A glucose measurement taken at any time. Diagnostic at 200 mg/dL or higher in someone with classic symptoms like extreme thirst, frequent urination, or unexplained weight loss.
The NIDDK overview of diabetes testing recommends confirming any positive result with a second test on a different day. Lab values can shift with illness, dehydration, or stress, and confirmation reduces the chance of misdiagnosis. This step often gets skipped, and it is worth asking about if your diagnosis was based on a single result.
Each test has trade-offs. A1C can be skewed by certain hemoglobin variants, anemia, or pregnancy. Fasting glucose can be misleading if someone ate within the prior 8 hours or is fighting an illness. The OGTT is more sensitive but takes longer and is harder to schedule. Our deeper guide to understanding your A1C results walks through how to read this number alongside everyday glucose values.
Tests That Distinguish Type 1 from Type 2
Once diabetes is confirmed, additional tests help separate type 1 from type 2 when the picture is not obvious. These second-tier tests are not always ordered automatically, but they should be considered any time the diagnosis is uncertain. The most useful are autoantibody panels and C-peptide measurement, and together they often clarify what the first round could not.
Autoantibody testing looks for the immune system markers behind type 1. The most commonly ordered are GAD (glutamic acid decarboxylase), IA-2 (islet antigen-2), ZnT8 (zinc transporter 8), and insulin autoantibodies. The presence of one or more strongly supports a type 1 diagnosis. Their absence supports type 2, although a small percentage of people with type 1 are antibody-negative at the time of testing.
C-peptide is a byproduct of insulin production, so it measures how much insulin your own pancreas is still making. Low or undetectable C-peptide points toward type 1, where beta cells have been destroyed. Normal or elevated C-peptide points toward type 2, where the pancreas is still producing insulin but the body is not using it well. Timing matters, because very high glucose can temporarily suppress beta cell output and make a type 2 result look more like type 1.
Why do these distinctions matter when both conditions raise blood sugar? Treatment paths diverge significantly. People with type 1 need insulin from the start of therapy, as covered in our overview of insulin therapy for type 1 diabetes. People with type 2 typically begin with lifestyle changes and oral medications before insulin enters the picture, as outlined in our piece on type 2 diabetes treatment options. Getting the type right at the start avoids months of treatment that does not match the underlying biology.
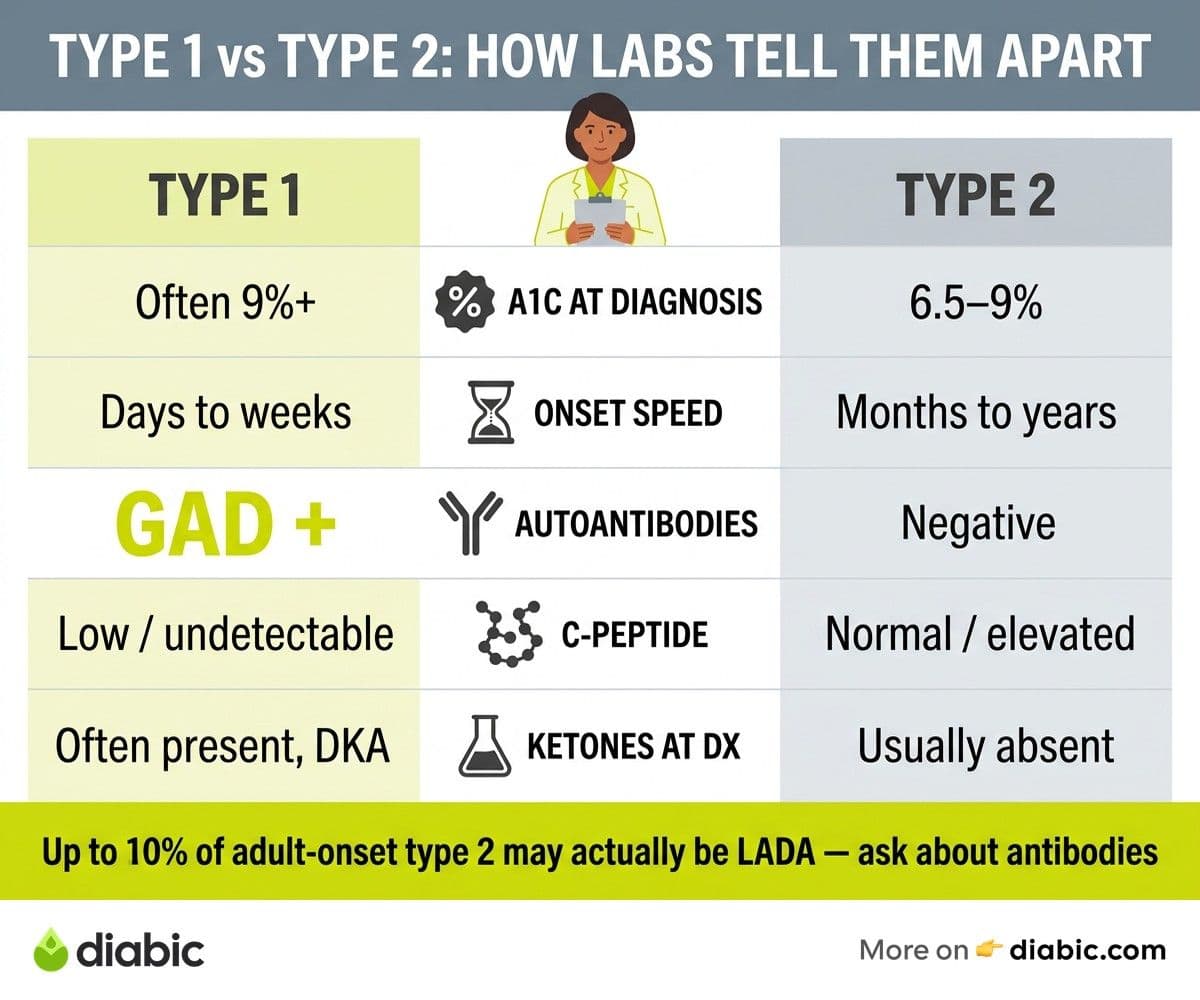
Comparison Table: How the Diagnostic Picture Differs
The table below pulls together the main differences in how type 1 and type 2 typically present at diagnosis. Real cases are messier than any chart, but this captures the patterns clinicians look for when sorting through ambiguous results.
A few caveats are worth highlighting. Body composition is not a reliable diagnostic marker on its own. Lean people develop type 2 diabetes, and people with type 1 can have any body type. Age is also not definitive, since around 40 percent of new type 1 cases occur in adults. Lab markers, especially antibodies and C-peptide, are far more reliable than physical appearance.
When the Diagnosis Is Uncertain: LADA, MODY, and Edge Cases
Not every case fits cleanly into type 1 or type 2. Latent autoimmune diabetes in adults (LADA) is sometimes called type 1.5. It is autoimmune like type 1 but progresses more slowly, and people with LADA can often manage on oral medications for months or years before needing insulin. Research published in Diabetes Care suggests that up to 10 percent of adults initially diagnosed with type 2 may actually have LADA. If oral medications start losing effectiveness unusually fast, autoantibody testing is worth requesting.
Maturity-onset diabetes of the young (MODY) is a group of inherited forms caused by single-gene mutations. MODY usually appears before age 25, often runs in multiple generations of a family, and does not involve autoimmune markers or significant insulin resistance. Genetic testing confirms the diagnosis. Distinguishing MODY matters because some forms respond well to specific oral medications and do not require insulin at all.
Pregnancy adds another layer. Gestational diabetes is screened with an OGTT, typically between weeks 24 and 28. The CDC's overview of diabetes testing covers screening guidance across these scenarios, including early pregnancy A1C testing for anyone with risk factors.
If your initial diagnosis does not feel like it fits, that instinct is worth raising with your provider. We have heard from readers who were told they had type 2, started on oral medications, watched their A1C climb anyway, and only got autoantibody testing months later. Talk to your doctor about whether antibody testing or C-peptide measurement makes sense in your situation, especially if treatment is not producing the results you expected.
What to Ask After You Receive a Diagnosis
A diagnosis appointment is rarely the moment when good questions come to mind. Walking out with a list of clarifying items for the next visit is one of the most useful things you can do for yourself. Here are the questions we hear most often from people who later said they wished they had asked earlier.
- Which type of diabetes do I have, and what tests confirmed that?
- Were autoantibody tests or C-peptide ordered, and if not, when might they be appropriate?
- What was my A1C at diagnosis, and what is the target we are aiming for?
- How often will I retest, and which tests will be repeated at each visit?
- What signs would suggest my treatment plan is not working as expected?
- Should anyone in my family be screened, and on what timeline?
For people initially told they have prediabetes, the same clarifying spirit applies. Understanding what prediabetes really means and which lab values define your starting point can change how you approach the next 12 months. Bring a notebook, ask for copies of your lab results, and make sure the answers you receive about type 1 vs type 2 diabetes match the numbers on the page.
Frequently Asked Questions
What is the difference between type 1 and type 2 diabetes on lab tests?
Type 1 typically shows positive autoantibodies (GAD, IA-2, ZnT8, or insulin autoantibodies), low C-peptide, and often a higher A1C at diagnosis with rapid symptom onset. Type 2 typically shows negative autoantibodies, normal or elevated C-peptide, and a slower, more gradual rise in A1C. Both are confirmed by the same first-line tests (A1C, fasting glucose, or OGTT), but the second-tier tests are what separate them clearly.
Can type 2 diabetes turn into type 1?
No. Type 2 cannot become type 1, because the two have different underlying causes. Some people with type 2 eventually need insulin as beta cell function declines over time, and that transition can feel like becoming type 1, but the biology is different. If oral medications stop working unexpectedly fast, ask your provider about autoantibody testing to rule out LADA, which is a slow-developing form of type 1 that is sometimes misdiagnosed as type 2.
How accurate are diabetes diagnostic tests?
Each test has a small error margin, which is why guidelines recommend confirming positive results with a repeat test on a different day. A1C can be affected by hemoglobin variants, anemia, or blood loss. Fasting glucose can shift with illness, dehydration, or stress. When tests disagree, autoantibodies and C-peptide add important context for distinguishing type 1 vs type 2 diabetes correctly.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Treatment & Medication
View all
Insulin Resistance Treatment Options Explained
Insulin resistance treatment is more than one pill. Here is a clear look at lifestyle, medication, and supplement options that actually work.

Insulin Resistance Diet: What to Eat and Avoid
An insulin resistance diet that fits real life. We cover foods that help, foods to limit, and meal patterns that improve insulin sensitivity.

Is Zepbound a Diabetes Medication? What You Need to Know
Is Zepbound a diabetes medication? We break down the FDA approval, the Mounjaro connection, and what tirzepatide means for blood sugar.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.