Diabetes Eye Exam Frequency: How Often to Go
Wondering about diabetes eye exam frequency? Here is how often to schedule a dilated exam by diabetes type, plus what to expect and how to overcome.

In this article(24)
Getting the right diabetes eye exam frequency on your calendar is one of the simplest, most effective things you can do to protect your vision. Eye exams catch problems before you notice symptoms, and early detection is what makes the biggest difference in long-term outcomes. The tricky part is that the rules shift depending on what type of diabetes you have, how long you have lived with it, and a handful of personal risk factors.
We get a lot of questions about whether yearly is really necessary, what happens during the exam, and what to do when cost or time gets in the way. This guide walks through the recommended schedule by diabetes type, the factors that may push you toward more frequent visits, and the practical ways to make eye exams a sustainable habit. Most of the guidance here lines up with the American Diabetes Association Standards of Care and the National Eye Institute.
Why Regular Eye Exams Matter with Diabetes
Diabetic retinopathy and macular edema are the two leading causes of vision loss tied to diabetes, and both can progress quietly. Many people assume their eyes are fine because they read just fine and have no pain or blurriness. The reality is that early retinal changes happen at the back of the eye, in tiny vessels you cannot see in the mirror or feel from the front.
By the time vision symptoms become obvious, damage may already be advanced enough to require injections, laser, or surgery to stabilize. Catching the same changes a year or two earlier often means a treatment plan focused on blood sugar, blood pressure, and monitoring rather than procedures. According to the NIDDK, early-stage retinopathy is highly responsive when caught before symptoms appear.
A dilated eye exam is the only routine way to see what is happening in your retina. Drops widen the pupil so the eye doctor can shine a light through and inspect the optic nerve, blood vessels, and macula. If you have ever wondered why your provider asks about blurred vision and diabetes at every visit, this is why. The eye exam is the visual confirmation behind those questions, and it can flag the earliest signs of diabetic retinopathy symptoms and stages long before you notice them yourself.
Recommended Diabetes Eye Exam Frequency by Type
The schedule that fits you depends on your type of diabetes and where you are in your timeline. The guidance below reflects current ADA and Mayo Clinic recommendations, but your eye doctor may adjust based on what they see.
Type 1 Diabetes
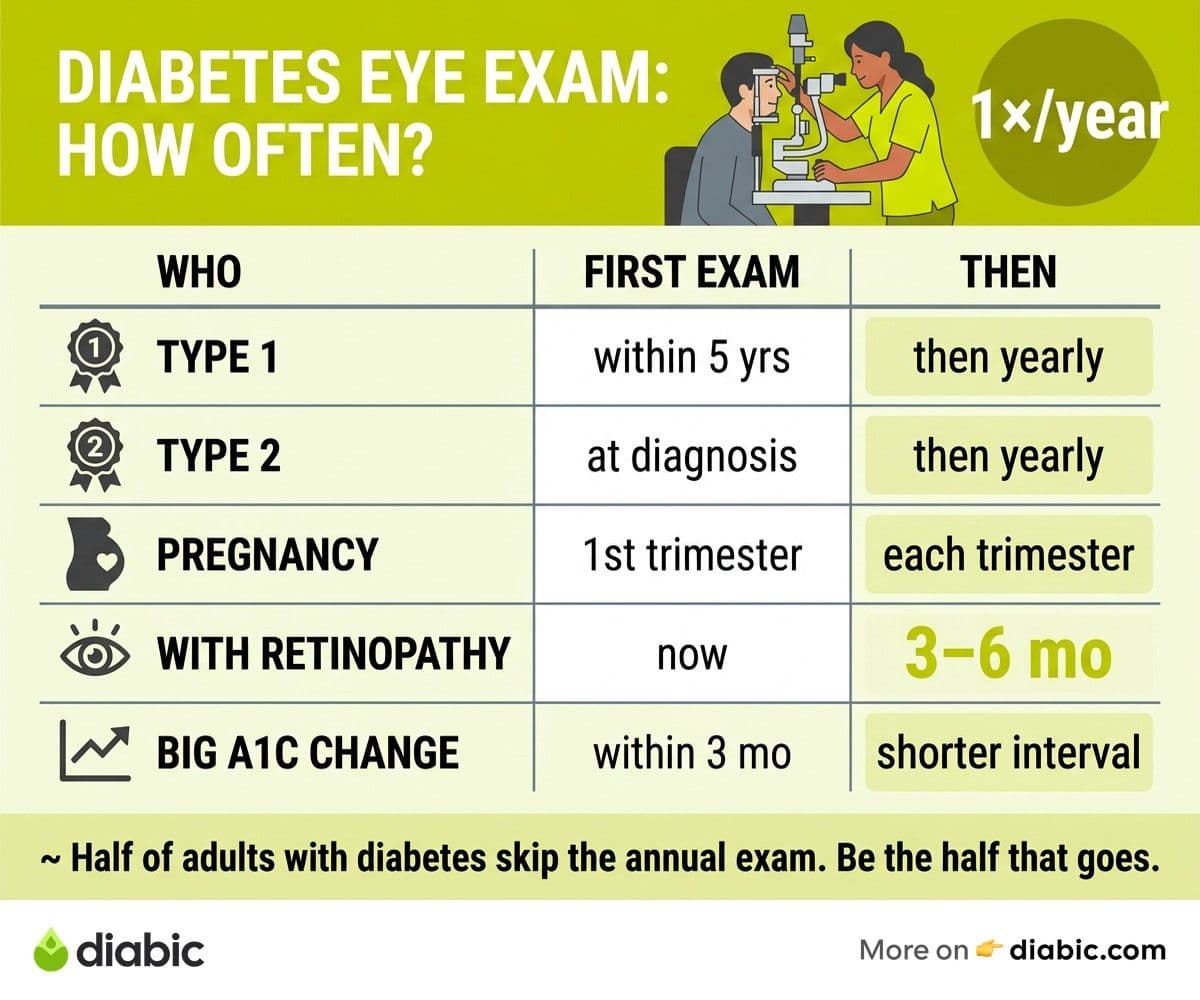
If you live with type 1 diabetes, the ADA recommends your first comprehensive dilated eye exam within five years of diagnosis. After that initial baseline, plan for an exam every year. Retinopathy is uncommon in the first few years of type 1, which is why the initial five-year window exists, but the annual cadence kicks in once that window closes.
Children diagnosed before puberty often follow a slightly different schedule, and your pediatric endocrinology team will guide that timing. For adults, the steady annual rhythm is what most studies have used to evaluate outcomes, so it is the schedule we anchor to.
Type 2 Diabetes
For type 2 diabetes, the recommendation is different because retinopathy can already be present at diagnosis. Many people live with elevated blood sugar for years before being formally diagnosed, which means damage may have started long before treatment did. The ADA recommends a comprehensive dilated eye exam at the time of diagnosis, then every year after.
If your first exam is clean and your blood sugar is well managed, your eye doctor may eventually stretch you to every two years. That decision should always come from your provider after reviewing your retinal images, not a self-decision based on feeling fine.
Gestational Diabetes and Pregnancy
Pregnancy adds a layer because hormonal shifts and rapid blood sugar changes can accelerate existing retinopathy. If you have pre-existing type 1 or type 2 diabetes and are planning pregnancy, an eye exam before conception or in the first trimester is standard. Follow-up exams during pregnancy and within the first year postpartum help catch any progression early.
Gestational diabetes (diabetes that develops during pregnancy) does not typically carry the same retinopathy risk, but if it persists or transitions to type 2 after delivery, the type 2 schedule kicks in.
Factors That May Change Your Schedule
Some people need more frequent monitoring than the baseline schedule suggests, and the difference between an annual and a six-month exam often comes down to what your provider sees on imaging. Here are the situations that commonly push the cadence shorter, and choosing between an ophthalmologist vs optometrist for diabetes can also matter when monitoring intensifies.
Existing Retinopathy or Macular Edema
If your last exam already showed signs of retinopathy, your eye doctor will likely shorten your interval to every three to six months. Early non-proliferative retinopathy is monitored closely so any progression can be caught before it threatens central vision. The same goes if you have a flag for diabetic macular edema, where fluid in the macula can change quickly and benefits from frequent OCT imaging.
Pregnancy with Pre-Existing Diabetes
Pregnancy with type 1 or type 2 diabetes typically means an exam each trimester, plus a postpartum follow-up. The combination of hormonal change, rapid metabolic shifts, and sometimes new insulin regimens can unmask or accelerate retinopathy that was previously stable.
Recent Big Changes in Blood Sugar Management
Starting insulin, transitioning to a pump, beginning a GLP-1 medication, or making a large diet change can all bring rapid A1C improvements. That sounds like good news, and over the long run it is, but in the short term a fast drop in A1C can trigger a temporary worsening of retinopathy in some people. If you have made a big shift in management in the past three to six months, mention it to your eye doctor so they can decide whether to bring you back sooner.
Other Risk Factors
High blood pressure, kidney disease, longer diabetes duration (more than 15 to 20 years), and a family history of severe retinopathy can all push your interval shorter. None of these are reasons to panic, but they are reasons to follow the schedule your eye doctor sets rather than the baseline annual default.
From my experience: After 14 years with type 1 diabetes, I have learned that my eye exam interval is not a static number. Some years I have been cleared at 12 months, and once, after a rough A1C swing, my retinal specialist asked me back in four. The first time that happened I was anxious, but it turned out to be a precaution, not a diagnosis. Now I see frequent monitoring as a sign my care team is paying attention, not a sign that something is wrong.
What Happens at a Diabetes Eye Exam
If you have not had a dilated exam before, knowing the steps removes most of the uncertainty. A typical appointment runs 60 to 90 minutes, including the time your pupils take to widen after the drops go in. The NEI walkthrough of dilated eye exams is a helpful primer if you want a step-by-step preview.
Visual Acuity and Pressure
The exam usually starts with a visual acuity test (the standard eye chart) and a tonometry test that measures pressure inside the eye. Tonometry takes a few seconds and feels like a quick puff of air or a soft probe touch, depending on the device. Eye pressure matters because people with diabetes have a higher risk of glaucoma.
Dilation
The eye doctor or technician puts in dilating drops, then asks you to wait 15 to 30 minutes for your pupils to widen. The drops sting for a moment and may make your near vision blurry and your eyes light-sensitive for a few hours afterward. This is the part most people dread, but it is short-lived and painless, and it is what makes the rest of the exam possible.
Retinal Imaging and Inspection
Once dilated, the eye doctor uses a bright light and lenses to look at the back of your eye. Many practices also take fundus photographs (color images of the retina) and OCT scans (cross-sectional images of the retinal layers). These images create a baseline that can be compared at every future visit, so even subtle changes get caught.
Driving Afterward
Plan for someone to drive you, or bring sunglasses and budget extra time before getting back behind the wheel. Most people feel comfortable to drive within three to four hours, but bright sunlight and screen reading can be uncomfortable until the dilation wears off.
Overcoming Barriers to Regular Eye Exams
If the schedule sounds straightforward but actually getting in the door feels harder, you are not alone. The CDC reports that roughly half of adults with diabetes do not get the annual eye exam they should, often because of cost, time, or fear. Here is how people in our community work around the most common barriers.
Cost and Insurance
Most U.S. medical insurance plans cover a yearly diabetic eye exam under your medical (not vision) benefits, which means it is often a flat copay rather than a separate vision plan charge. If you do not have insurance, federally qualified health centers, hospital clinics, and programs like EyeCare America offer reduced-cost or free exams. Telemedicine retinal screening, often available through your primary care or endocrinology clinic, can also provide a covered baseline if a full in-person exam is out of reach.
Time Constraints
The 60 to 90 minute appointment, plus dilation recovery, makes scheduling feel heavier than a quick visit. Booking the first or last appointment of the day, asking whether the practice can do imaging without dilation as a screening option, and stacking the appointment near another errand can all reduce the perceived time cost.
Fear or Discomfort
Dilation drops, bright lights, and the air puff test are not most people's favorite, but they are short and not painful. If you find them stressful, tell the technician. They can warn you before each step and pause if you need a moment.
Telemedicine Retinal Screening
A growing number of primary care offices and endocrinology clinics now offer in-house retinal cameras that can capture images without dilation. A board-certified retinal specialist reads the images remotely and flags anything that needs follow-up. This is not a full replacement for a comprehensive in-person exam, but it can be a strong first-line screening, especially if scheduling with an eye doctor is hard.
Building eye exams into your diabetes care calendar matters more than scheduling them perfectly. Pairing your eye exam booking with your annual labs or a birthday reminder, or with simple diabetes eye care tips you already follow, helps keep diabetes eye exam frequency from sliding off your radar. When eye exams become as automatic as your dental cleaning, the long-term protection compounds.
FAQ
How often should people with diabetes get eye exams?
For most adults with diabetes, an annual dilated eye exam is the standard. People with type 1 diabetes start within five years of diagnosis, while people with type 2 begin at the time of diagnosis. Your eye doctor may shorten the interval if you already have retinopathy, are pregnant, or have other risk factors.
Do people with type 2 diabetes need yearly eye exams?
Yes. Type 2 diabetes can cause retinal changes before you notice any symptoms, and it may have been silently affecting your eyes before you were diagnosed. An annual exam is the baseline, and your eye doctor may extend that to every two years only after multiple clean exams and stable blood sugar.
What if I have no vision symptoms, do I still need an eye exam?
Yes. Most early diabetic eye disease has no symptoms, which is exactly why screening matters. Waiting for blurriness, floaters, or vision loss to appear means waiting until damage has already progressed. The whole point of a steady diabetes eye exam frequency is to catch changes before you feel them.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Rezwana Parvin Rumpa is an obstetrics and gynaecology specialist with clinical focus on gestational diabetes, PCOS, and fertility. She holds the MRCOG (Final Part) from the Royal College of Obstetricians and Gynaecologists in London, the MRCPI (Final Part) from the Royal College of Physicians of Ireland, and an MBBS from Shaheed Monsur Ali Medical College under Dhaka University. Dr. Rumpa serves as a Senior Medical Officer in the Obs and Gynae department at BRB Hospitals Ltd, where she has spent three years managing prenatal care, emergency obstetric cases, and women's-health surgery. On Diabic, she medically reviews content for women living with diabetes, with particular attention to pregnancy, PCOS, and reproductive-health intersections.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.