Switch From Insulin Injections to a Pump? How to Choose
Insulin injections vs pump comparison: pros, cons, costs, and a decision framework to help you choose the right insulin delivery method.

In this article(17)
The insulin injections vs pump decision is one of the bigger choices you will make in diabetes management, and there is no universally correct answer. Both approaches deliver the same medication, both can produce excellent A1Cs, and both have honest trade-offs that show up in daily life rather than in clinical trials.
This guide walks through how multiple daily injections (MDI) and pump therapy actually compare in practice. The pros and cons are real on both sides. By the end, you should have a framework to decide whether switching makes sense for you, whether staying on MDI is the smarter call, or whether a smart pen sits in the middle as a better fit.
If you are newly diagnosed and trying to understand pump therapy from scratch, our insulin pump guide covers the basics first.
Insulin Injections vs Pump: How They Compare
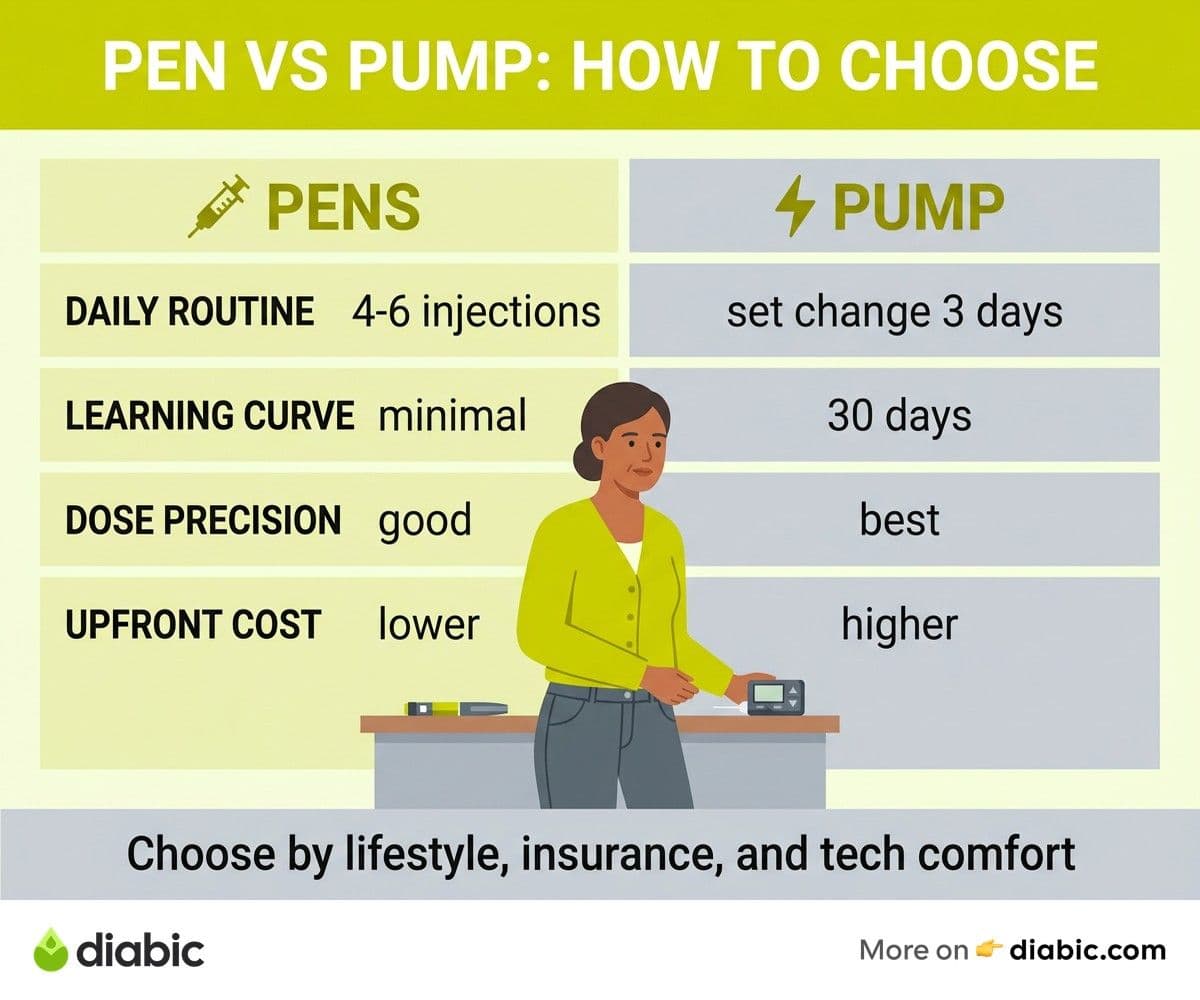
Multiple daily injections deliver basal insulin through a once or twice daily long-acting insulin (Lantus, Tresiba, Basaglar) plus rapid-acting insulin (Humalog, Novolog, Fiasp) at meals and corrections. Most people on MDI take 4 to 6 injections per day with insulin pens or syringes.
Pump therapy delivers a single rapid-acting insulin continuously through a small device worn on the body, with a thin cannula inserted under the skin every 2 to 3 days. The pump replaces both your basal injection and your mealtime injections by programming a continuous background rate plus on-demand boluses.
The two delivery methods produce similar average A1C results across populations, but the variance and the daily experience differ significantly. Here is how the head-to-head looks.
The American Diabetes Association includes both delivery methods as recommended options in its Standards of Care, and the choice between them is meant to be individualized based on goals, lifestyle, and patient preference.
Benefits of Switching to an Insulin Pump
The benefits of insulin pump therapy show up most clearly for people whose MDI regimen is producing variability they cannot smooth out. A pump is not magic, but it gives you tools that pens cannot match.
The biggest benefit is basal precision. Long-acting insulin like Tresiba lasts 24 hours but releases at a roughly fixed rate. Real bodies do not have fixed insulin needs across the day. Most people need more insulin in the early morning (the dawn phenomenon) and less in the early evening or during sleep. A pump can program different basal rates hour by hour to match those patterns. MDI can only approximate.
A meta-analysis from Pickup and Sutton in BMJ (2005) compared pump therapy to MDI across multiple randomized trials and found A1C reductions of about 0.4 percentage points with pump use, plus reductions in severe hypoglycemia. Subsequent studies with modern AID systems have shown larger benefits, particularly for time-in-range and overnight glucose stability.
What the Daily Experience Looks Like
Pump users typically take one site change every 2 to 3 days instead of 4 to 6 injections per day. The math is roughly 14 to 21 injections per week on MDI compared to 2 to 3 site changes per week on a pump. The needles are also smaller and the insertion is faster than a manual injection.
Bolus flexibility is the other day-to-day win. Pumps support extended boluses that deliver insulin over 30 minutes to 8 hours, which helps with high-fat meals like pizza or pasta. Dual-wave boluses split the dose between an immediate hit and an extended tail. Micro-corrections of 0.05 to 0.5 units are easy with a pump and impossible with a pen.
For overnight management, a pump with a closed-loop algorithm and a CGM can adjust basal delivery automatically based on glucose trends. This is the single biggest reason many pump users wake up in range more often than they did on MDI. Our insulin pump costs post breaks down the financial side of these benefits.
Disadvantages of Insulin Pump Therapy
Pump therapy has real downsides, and ignoring them does no one any favors. Which of these is a disadvantage of insulin-pump technology that matters most to you depends on your priorities and your tolerance for device wear.
A pump means a device attached to your body 24 hours a day, 7 days a week. For some people that fades into the background within weeks. For others it never stops feeling intrusive. There is no way to know which group you fall into until you try, though most pump-curious people who actually start therapy adapt to the wear factor within a month or two.
Site infections, adhesive reactions, and skin breakdown are real risks at the infusion site. Most are minor and preventable with good hygiene, but they happen. Our insulin pump site infections prevention guide covers the routine that keeps these issues rare.
Equipment and Backup Plans
Pumps fail. Sets clog. Tubing kinks. Batteries die. Reservoirs run empty at inconvenient times. Pump users have to maintain a backup MDI plan with both basal and rapid-acting pens, know how to convert pump settings into injection doses, and be prepared to switch within an hour or two if the pump goes down.
This backup planning is a real cognitive load that MDI users do not carry. If the idea of always having a Plan B in your bag feels exhausting, MDI may suit you better.
Cost and Learning Curve
The upfront cost of a pump is significant even with insurance. Out-of-pocket expenses range from a few hundred dollars to several thousand dollars depending on your DME benefit. Ongoing supply costs add roughly $100 to $300 per month for sets, reservoirs, and CGM sensors. MDI supply costs (pen needles, lancets, glucometer strips) tend to be substantially lower, even with the same insulin prescriptions.
The learning curve is also real. Programming basal rates, setting carb ratios and correction factors, learning to manage extended boluses, and getting comfortable with closed-loop algorithms takes weeks to months. Most clinics provide pump training over 2 to 4 sessions, but the practical fluency comes from daily use.
When Insulin Injections Are the Better Choice
MDI is not a fallback. For some people it is the right choice on its own merits, and a clinic that pushes everyone toward a pump is not serving those patients well.
People who prefer device-free simplicity are often happier on MDI. If the idea of always wearing a pump bothers you, that bother does not go away. It also affects partners, body image, and clothing choices in ways that pump enthusiasts sometimes underestimate.
People with sensitive skin who react to medical adhesives may struggle to wear a pump comfortably. Repeated adhesive reactions can make pump therapy genuinely worse than MDI in terms of quality of life, and some people simply do not tolerate the materials no matter what barrier products they try.
Active Lifestyles and Specific Sports
Some athletes prefer MDI because a pump introduces variables that get in the way of training and competition. Contact sports, swimming, and gymnastics all create wear-time challenges. Endurance athletes have different concerns: extended exercise often requires basal reductions that a pump can do precisely, but it also means a device on the body for many sweaty hours.
There is no single right answer here. Most pumps are fine for most athletes, but a small number of competitive athletes choose MDI specifically to keep training sessions device-free.
Budget and Insurance Constraints
If your insurance does not cover a pump, or covers it with a high coinsurance share, the financial math may not work. The American Diabetes Association maintains insurance navigation resources that can help, and patient assistance programs through pump manufacturers reduce costs for some patients. But MDI remains substantially cheaper out of pocket for most people, and that matters.
UK-based readers should look at the NICE guidelines on insulin pump therapy, which set specific clinical criteria for NHS coverage. The criteria include severe hypoglycemia despite optimized MDI and inability to achieve target A1C without disabling lows.
How to Decide: Questions to Ask Yourself and Your Doctor
The right decision usually surfaces from a small set of questions, asked honestly. Here is the framework we use with people who are weighing the switch.
Start with your current numbers. What is your most recent A1C, and how does it compare to your goal? What is your time-in-range from CGM data over the past 30 days? How often do you have lows below 70, and how many have been severe? If your current management is producing the outcomes you want, the case for switching is weaker.
Next, assess how MDI feels day to day. Are you comfortable with 4 to 6 injections, or are some of them being skipped? Is your basal insulin pattern mismatched with your needs (high fasting glucose despite an evening Lantus dose, for example)? Are you struggling with high-fat meals, exercise variability, or overnight glucose? Pumps solve specific MDI pain points, not all problems.
Ask about wearability. Are you open to a device on your body 24/7? Are you OK with a tubed pump on your hip or a tubeless pod on your arm or abdomen? Have you handled a demo pump in clinic? Wearing a saline-filled pump for a week before committing to a real one is increasingly available and worth asking about.
Insurance and Cost Questions
Bring concrete questions to your insurance navigator or diabetes educator:
- What is my DME deductible and coinsurance for an insulin pump?
- How long is the prior authorization process at this clinic?
- Which pumps does my plan prefer or restrict?
- What are the supply costs once I am on a pump, and are CGM sensors covered through pharmacy or DME?
Compare those answers to your MDI supply costs. If the gap is small and the clinical case is strong, the switch makes sense. If the gap is large and the clinical case is weak, MDI plus a CGM may be the better path.
For a different angle on this decision, our OmniPod review covers the tubeless option specifically, since some people who decide against a tubed pump are still good candidates for a pod.
Smart Insulin Pens: A Middle Ground
Smart insulin pens have closed some of the gap between MDI and pump therapy in recent years. These connected pens (InPen, Tempo Pen, NovoPen 6) track every dose automatically, sync with CGM data, and offer dose calculators in companion apps.
A smart pen does not replicate basal precision or extended boluses, but it does eliminate one of the biggest MDI pain points: forgotten doses and missed log entries. The app-based dose calculator also helps with carb-to-insulin ratios and active insulin tracking, both of which were previously pump-only features.
For people who want better MDI but are not ready for a pump, a smart pen is often the right next step. Our smart insulin pens post covers the available options and how to pick one.
When a Smart Pen Might Be All You Need
A smart pen may be enough if you are doing reasonably well on MDI, your main issue is dose tracking and forgetting boluses, and you have a CGM that you trust. The combination of a CGM plus a smart pen gives you many of the data benefits of pump therapy without the device wear or the complexity.
If you go this route and find that your time-in-range is not improving or your variability stays high, that is useful information. It may be a sign that pump therapy is the right next step, and you will arrive at that decision with better data than if you had stayed on basic MDI.
From my experience: I switched from MDI to a pump 9 years into my type 1 diagnosis, and the first month felt worse than the last month on injections. The learning curve was real. Six months in, my time-in-range was clearly better, my dawn phenomenon was finally manageable, and I felt the difference. But I would not say it is for everyone. A close friend who has had T1D for the same length of time stayed on MDI plus a smart pen and a CGM, and his outcomes are nearly identical to mine. The right tool is the one that fits your life.
FAQ
Should I switch from insulin injections to a pump?
Switch from insulin injections to a pump if your MDI regimen is not getting you to your A1C and time-in-range goals, you have frequent dawn phenomenon highs or overnight lows, you struggle with high-fat meals or variable exercise, or you are tired of carrying multiple insulin pens. Stay on MDI if your numbers are where you want them, you cannot tolerate a device on your body, your insurance coverage makes a pump unaffordable, or you have skin sensitivities that make adhesive wear painful. Talk to your doctor about whether your specific situation favors one path.
Which is better, insulin injections or a pump?
Neither is universally better. Insulin pumps offer more precise basal delivery, fewer daily injections, better overnight glucose control, and flexible bolus options like extended doses for high-fat meals. Insulin injections are simpler, cheaper, device-free, and easier to back up if equipment fails. Research suggests pump therapy produces modest A1C improvements and reduces severe hypoglycemia, but the day-to-day experience differs in ways that matter to individual patients. The right choice depends on your goals, your lifestyle, and your tolerance for device wear.
Can you go back to injections after using a pump?
Yes, you can switch back to insulin injections after using a pump. Your endocrinologist will help you convert your pump basal rates and bolus settings into a long-acting insulin dose plus mealtime rapid-acting doses. Some people switch back temporarily during pregnancy, surgery, or extended travel, while others switch back permanently because they prefer MDI. The transition typically takes 1 to 2 weeks of dose tuning to stabilize.
The insulin injections vs pump decision is rarely permanent and rarely about which approach is medically superior. It is about which one fits your life right now, and that may change as your situation, your insurance, and your goals evolve.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Devices & Technology
View all
Using a Continuous Glucose Monitor for Hypoglycemia
A continuous glucose monitor for hypoglycemia can catch lows before symptoms hit. Learn how alerts, trends, and CGM data help prevent severe episodes.

Best Continuous Glucose Monitors for Type 2 Diabetes in 2026
Compare the best continuous glucose monitor for type 2 diabetes options, including Stelo, FreeStyle Libre 3, and Dexcom G7, with pricing and accuracy.

Best Blood Glucose Meters for Home Testing in 2026
Compare the best blood glucose meter options for home testing in 2026, including accuracy ratings, strip costs, and features that matter day to day.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.