Teen Diabetes Mental Health: Spot the Burnout
Teen diabetes mental health matters. Spot the signs of burnout vs depression, learn what helps, and know when to bring in professional support.

In this article(9)
When a teenager who used to check their blood sugar without being asked starts skipping doses, hiding their meter, or saying "I just don't care anymore," it is not rebellion. It might be diabetes burnout, and recognizing it early can prevent both physical and emotional harm. Teen diabetes mental health is one of the most underdiscussed parts of pediatric care, and the families who address it head-on tend to come through with stronger relationships and steadier glucose data.
Burnout is common, predictable, and treatable. Teen diabetes mental health rarely fails on its own; it slides slowly, then all at once. Spotting it before it becomes a crisis usually means catching small signs that are easy to dismiss as moodiness or laziness. The signs are real. The fix involves both practical changes and the right support.
What Teen Diabetes Burnout Looks Like
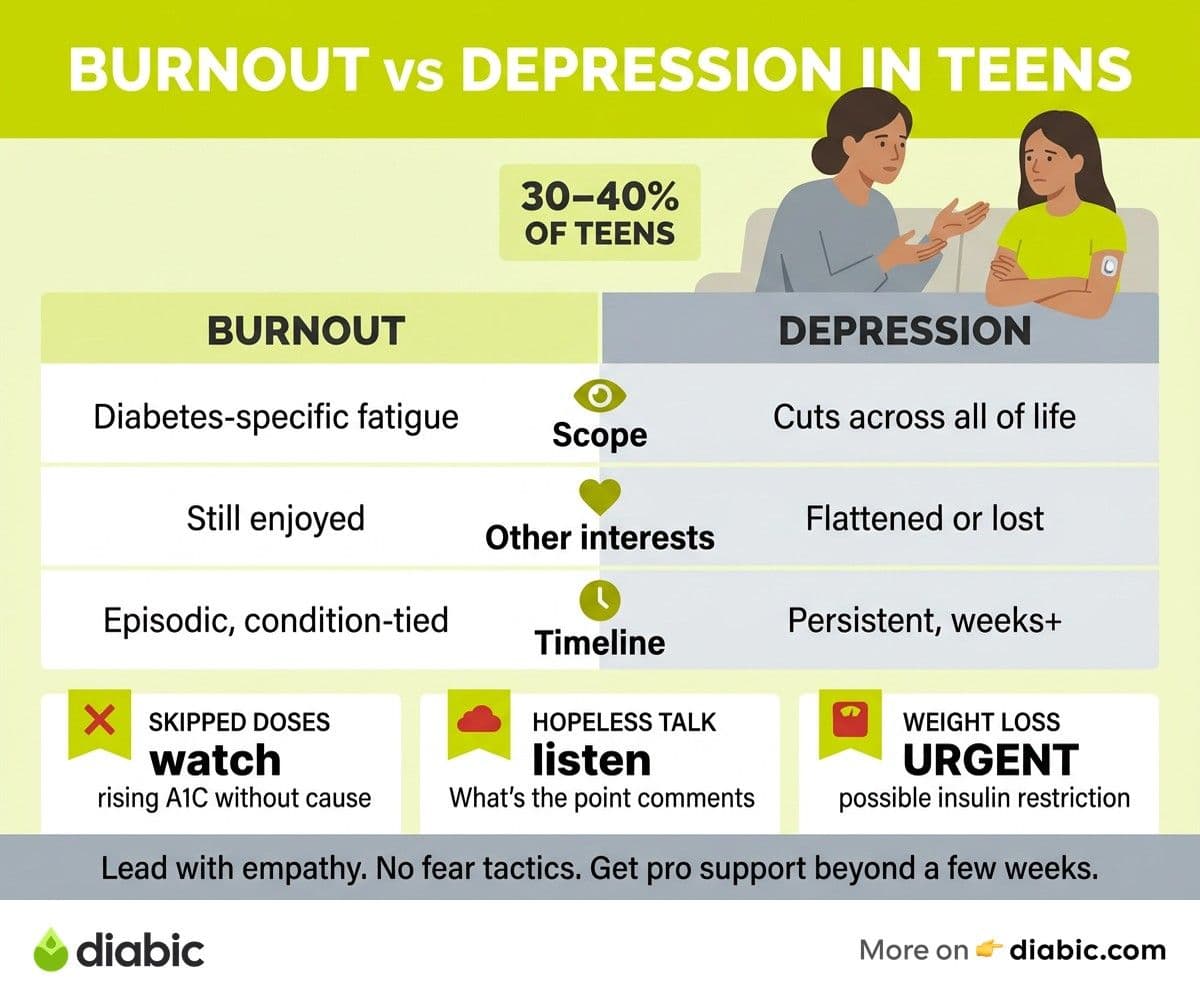
Diabetes burnout in adolescents shows up in a recognizable pattern. Research published in journals like Diabetes Care suggests roughly 30 to 40 percent of teens with type 1 experience meaningful burnout at some point.
The most common signs:
- Skipping blood sugar checks or insulin doses. A teen who used to test before lunch suddenly does not. CGM applications get delayed. Bolus doses get missed and corrections climb.
- Avoiding diabetes conversations. Eye-rolls, one-word answers, or shutting down when you bring up appointments, glucose readings, or supplies.
- Hopelessness statements. "Nothing I do makes any difference." "What's the point." "I just want to be normal." These deserve attention even if they sound like throwaway lines.
- Hiding devices and data. Putting the CGM under clothes specifically to avoid questions. Closing apps when you walk in. Refusing to share readings.
- A1C climbing or glucose patterns becoming erratic without an obvious cause like a growth spurt or illness.
- Weight loss without explanation. This can be a sign of intentional insulin restriction (sometimes called "diabulimia"), which is a serious eating disorder requiring immediate intervention.
Burnout is not a character flaw. It is the predictable response to a relentless demand. Teens are asked to do daily math, manage chronic uncertainty, and make perfect decisions about food and dosing in social situations where their friends never have to think about any of it. The wonder is not that some hit a wall. The wonder is that so many do not.
Our broader piece on diabetes in teenagers covers the developmental context. This post focuses on what to do when burnout has set in.
Burnout vs Depression: Know the Difference
Burnout and depression can look similar on the surface, but they are distinct, and they sometimes coexist. The American Psychological Association and most diabetes mental health specialists draw the line this way.
Diabetes burnout is condition-specific. The teen is fed up with diabetes. They may still enjoy their friends, their hobbies, school, sports. They are functional in other areas of life but exhausted by the daily demand of glucose monitoring, dose calculations, and food awareness. The frustration is real and rational, not a sign of underlying mental illness.
Depression affects all areas of life. Sleep changes (too much or too little), appetite changes, loss of interest in activities they used to enjoy, persistent low mood, withdrawal from friends, hopelessness that extends beyond diabetes. Depression is a clinical condition that benefits from professional treatment.
The two can trigger each other. Untreated burnout can spiral into depression. Depression can make burnout feel insurmountable. Our adult-focused guide to diabetes burnout in adults and our piece on diabetes distress vs depression explain the distinction in more depth, and the framework applies to teens too.
A mental health screening from your endocrinology team or a pediatric psychologist can help distinguish between the two. Many pediatric endo offices now use brief screening tools at routine visits. If yours does not, ask. The PHQ-A (Patient Health Questionnaire for Adolescents) and the PAID-T (Problem Areas in Diabetes for Teens) are both validated and quick.
How Parents Can Help Without Making It Worse
The temptation when you see your teen sliding is to push harder. The result is almost always the opposite of what you want. The pushback grows, the relationship suffers, and the burnout deepens. A different approach works better.
Lead with empathy first. "I can see this is really hard right now." "I'm sorry you have to deal with this." "Tell me what feels hardest about it." Spend at least one full conversation listening before you propose any solution. The teen needs to know you understand before they will hear advice.
Avoid guilt and fear tactics. "You'll damage your kidneys if you skip doses." "Do you want to go blind?" These threats land as criticism, not motivation. They increase shame, which increases avoidance, which increases the behavior you were trying to stop. The American Diabetes Association's psychosocial care position explicitly recommends against fear-based messaging in adolescents.
Offer to take back some management tasks temporarily. "What if I take over carb counting at dinner this week?" or "I can text you reminders to bolus, just say yes or no when I do." Reducing the load is sometimes the most useful thing a parent can do. It signals support, not surveillance.
Suggest a break from perfectionism. Aim for "good enough" not flawless. Time in range of 50 percent is not a failure when it used to be 75 percent. The recovery from burnout starts with achievable wins, not by demanding return to peak performance.
Watch for warning signs that need urgent attention. Severe weight loss, intentional insulin restriction, expressions of self-harm, persistent hopelessness, complete withdrawal, these warrant immediate professional support, not a wait-and-see approach.
From my experience: After more than a decade with diabetes, the moments I needed support most were the moments my parents asked me what would help instead of telling me what to do. Even at 16, "what do you need from me right now?" landed differently than "you need to test your blood sugar." The same words, hours apart, can build trust or burn it down. The teens I have talked with since echo this almost word for word.
Teen Diabetes Mental Health: When Professional Help Is Needed
If burnout lasts more than a few weeks or starts shading into depression, professional support helps faster than family effort alone.
Diabetes-specific therapists. Many endocrinology offices have a behavioral health specialist on staff or can refer one. Therapists who specialize in chronic illness understand the unique cognitive load of diabetes management and do not need the basics explained. Ask your endo team for a referral; the JDRF mental health resources include directories of qualified providers.
Peer support. Connecting your teen with other teens who have diabetes is one of the highest-impact interventions. Diabetes camps, JDRF teen events, and ADA-sponsored meetups create community. Online groups (heavily moderated, age-appropriate) work for teens who cannot attend in person. Our guide to diabetes support groups covers options across age groups.
Technology that simplifies the routine. Sometimes the burnout is partly mechanical. A teen on multiple daily injections may benefit from switching to an automated insulin delivery (AID) system like the Omnipod 5, t:slim X2 with Control-IQ, or Medtronic 780G. The reduced burden of constant dose math can lift months of accumulated frustration. This is a conversation for your endo team, not a solo decision.
Family therapy. When burnout has strained the parent-teen relationship, a few sessions with a family therapist familiar with chronic illness can reset the dynamic. The teen learns to express what they need; the parent learns where the line between support and control should sit.
Crisis support. If you ever suspect intentional insulin restriction, an active eating disorder, or any expression of suicidality, call your endo team and your child's primary care provider the same day. The 988 Suicide and Crisis Lifeline is available 24/7. These are medical emergencies, not parenting failures.
FAQ
What are the signs of diabetes burnout in teenagers?
Common signs include skipping blood sugar checks or insulin doses, avoiding conversations about diabetes, expressing hopelessness, hiding devices or data, and a noticeable rise in A1C without an obvious cause. Weight loss without explanation can signal intentional insulin restriction, which is a serious sign that needs immediate attention.
How do I help a teen with diabetes depression?
Start with professional support. Ask your endocrinology team for a referral to a therapist familiar with chronic illness, ideally one with diabetes experience. At home, lead with empathy, avoid guilt-based messaging, take back some management tasks if your teen needs the load reduced, and watch for warning signs that need urgent care. Connect them with other teens who have diabetes through camps, online communities, or peer programs.
Can diabetes burnout in teens go away on its own?
Sometimes mild burnout resolves with a break, an honest conversation, and small changes to the management routine. More serious burnout (lasting weeks or months, or accompanied by skipped doses and rising A1C) usually does not resolve on its own and benefits from professional mental health support, family adjustments, and sometimes technology changes that simplify the daily burden.
What is diabulimia and how is it different from burnout?
Diabulimia is the deliberate restriction of insulin to lose weight. It is a serious and life-threatening eating disorder, not just a form of burnout. Signs include rapid weight loss, persistent high blood sugar despite seemingly adequate food intake, recurrent DKA, and obsessive focus on weight or body image. It requires immediate, specialized treatment from a team that includes both endocrinology and eating disorder specialists.
When you take teen diabetes mental health seriously, you give your child a much better shot at carrying their diabetes into adulthood with confidence rather than resentment. The numbers will recover. What matters more is that the relationship and the trust survive the rough patch.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Living with Diabetes
View all
Generic vs Brand Insulin: Is There a Difference?
Generic vs brand insulin compared: how biosimilars are approved, what you save with Semglee or ReliOn, and how to talk to your doctor about switching.

Patient Assistance Programs for Diabetes Medication
Patient assistance programs diabetes patients qualify for can cut prescription costs to little or nothing. Here is how to find and apply for them.

Diabetes Supply Savings Tips That Actually Work in Real Life
Practical diabetes supply savings tips for cutting costs on test strips, CGMs, insulin, and pump supplies without compromising your care.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.