Recognizing Diabetic Neuropathy in Feet (With Pictures)
Pictures of diabetic neuropathy in feet help you spot early signs. Learn what color shifts, calluses, ulcers, and numbness mean, plus what to do next.

In this article(16)
The first signs of diabetic foot neuropathy rarely arrive as pain. They show up quietly: a callus that builds in a new spot, a patch of skin that looks slightly redder than the foot beside it, a sock that comes off with a fleck of blood you do not remember earning. Pictures of diabetic neuropathy in feet matter because the eye catches changes that sensation may have already stopped reporting.
This guide walks through what early neuropathy looks like, what it feels like (or fails to feel), and how to do a careful self-exam at home. Where photographs would normally appear, we describe each visual sign in detail so you know exactly what to look for in your own feet or in clinical reference images. The aim is to give you the language and the pattern recognition to catch problems while they are still small.
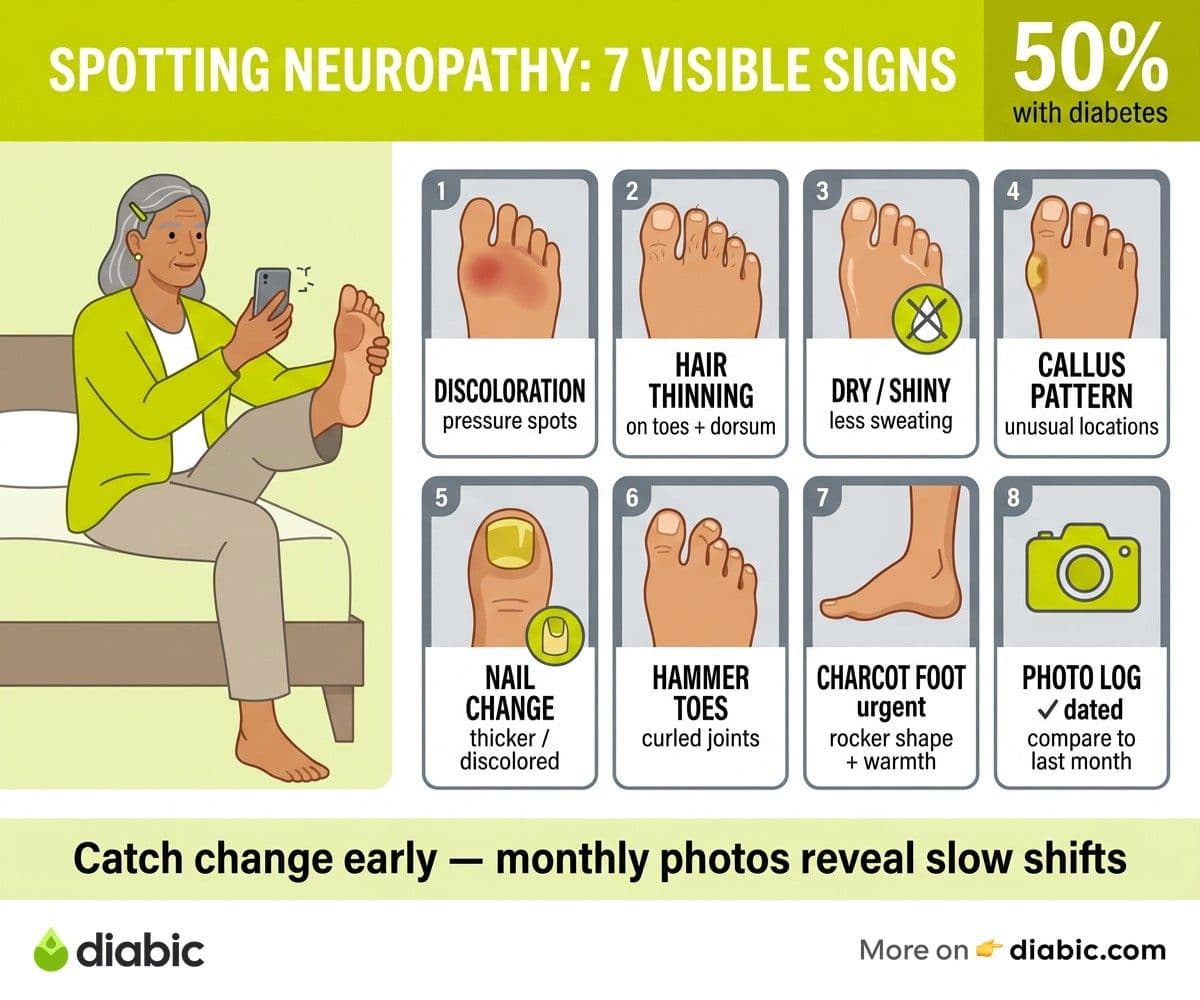
Diabetic neuropathy is common, progressive, and very preventable in its later stages when caught early. According to the National Institute of Diabetes and Digestive and Kidney Diseases, about half of people with diabetes will develop some form of nerve damage during their lifetime, and the feet are usually the first place it appears.
What Diabetic Neuropathy Looks Like in the Feet
Pictures of diabetic neuropathy in feet usually show a combination of subtle and dramatic changes. The subtle changes are what most people miss, and they are also where prevention has the biggest payoff. Skin discoloration is among the earliest signs. Areas of the foot that bear unusual pressure may look pinker or redder than the surrounding skin, almost like a faint bruise that does not fade. In darker skin tones the change may show as a deeper brown or purple patch, and in lighter skin tones it can read as ruddy or shiny.
Image alt-text intent: a top-down view of a foot showing a faint reddish discoloration along the ball under the second and third toes, with surrounding skin appearing normal, suggesting early pressure-related changes from altered gait.
Hair patterns shift too. Healthy feet usually have fine hairs across the tops of the toes and the dorsum, the upper surface of the foot. With reduced circulation and nerve signaling, those hairs thin out or disappear, leaving the skin smooth and sometimes shiny. The change is gradual, so people often only notice when comparing recent photos to older ones.
Nails change as well. They may grow thicker, more brittle, or take on a yellow or grey tint. Vertical ridges deepen, the nail bed lifts at the edges, and fungal infections become more frequent because the immune environment under the nail shifts. Trimming becomes harder, which is part of why podiatrists ask people with neuropathy not to cut their own nails once changes appear.
Skin texture changes round out the visual picture. Reduced sweating is one of the early effects of autonomic neuropathy, and dry, flaking skin is the visible result. Cracks form at the heels, between the toes, and along pressure points. Those cracks are where ulcers often start, especially if the person cannot feel the discomfort that would normally signal a problem.
Pictures of Diabetic Neuropathy in Feet: Visible Signs to Know
Calluses in unusual patterns
A callus is the body's response to repeated pressure or friction. In a foot with normal sensation, calluses form in predictable spots like the ball of the foot or the back of the heel. In a foot with neuropathy, calluses build in odd places because the person walks differently without realizing it, putting weight on areas that were not designed to bear it.
Image alt-text intent: close-up of a thickened, yellowed callus on the lateral edge of the big toe, with surrounding skin appearing dry, indicating altered weight bearing common in diabetic peripheral neuropathy.
Look for thick, yellow, or hardened patches anywhere along the sole, the sides of the toes, or the tops of toes that rub the inside of shoes. A callus that bleeds when scraped, or that has a dark spot in the center, may have a small ulcer hiding underneath and needs professional attention.
Toe deformities
As the small muscles in the foot weaken, toes start to curl. Hammer toes bend at the middle joint, claw toes bend at both joints, and the tips of the toes may end up pressing into the floor while the tops rub against the shoe. The visual signature is unmistakable once you have seen it, and reference images from sources like Mayo Clinic and the American Podiatric Medical Association make the pattern easier to spot.
These deformities are not just cosmetic. They change how shoes fit, where calluses build, and how easily ulcers form on the new pressure points. Custom orthotics or therapeutic footwear, recommended by a podiatrist, can offload these areas and reduce ulcer risk.
Charcot foot and arch changes
Charcot foot is a more advanced complication where bones in the midfoot weaken and collapse, often after an unnoticed fracture. The foot may look rocker-bottomed, swollen, warm to the touch, and red. It can be mistaken for an infection or a sprain. Anyone with neuropathy who notices new swelling, warmth, or a sudden change in foot shape should be seen the same day, as early treatment can preserve the foot architecture.
Image alt-text intent: a side profile of a foot showing a flattened arch with the midfoot bulging downward, redness across the top, and visible swelling, characteristic of acute Charcot foot.
Ulcers and breakdown
Ulcers usually start small, often as a blister, callus, or scratch the person did not feel. They progress to open wounds that may weep clear or yellow fluid, and they often appear on the ball of the foot, under a bony prominence, or between toes. A black or grey edge around an ulcer suggests tissue death and is an emergency. Our piece on diabetic foot ulcer treatment covers what proper wound care looks like.
Diabetic Peripheral Neuropathy: Signs You Can Feel (Or Cannot Feel)
The hallmark of diabetic peripheral neuropathy is symmetry. Symptoms usually start in both feet at once, in a "stocking" pattern that begins at the toes and slowly extends upward over years. Asymmetric symptoms, where one foot is dramatically different from the other, suggest a different problem and should be evaluated separately.
Numbness is the most common sensation, or rather the absence of one. People often describe it as "walking on cotton" or feeling like they have a thick sock on when they do not. The danger of this symptom is that it removes your protective alarm system. A pebble in the shoe, a too-hot bath, or a sharp object underfoot may go unnoticed until damage has already been done.
Tingling, burning, and pins-and-needles sensations come and go in early neuropathy and tend to worsen at night for many people. Some describe a feeling of crawling ants, electric shocks, or icy water on the skin. These positive symptoms (sensations that should not be there) often coexist with negative symptoms (loss of normal feeling) in the same patient.
Paradoxically, some people develop heightened sensitivity. Light touch from a bedsheet, sock, or breeze can feel painful. This is called allodynia, and it is more common in established neuropathy. Our guide to diabetic neuropathy foot pain and relief goes deeper into pain management strategies.
Balance changes are an underrecognized symptom. The feet send constant proprioceptive signals to the brain about ground texture, slope, and stability. When those signals fade, balance suffers. Many people with neuropathy notice they trip more often, struggle on uneven ground, or feel unsteady in the dark. Falls are a real risk, and addressing balance early through physical therapy can help.
If you want a broader review of how neuropathy presents across the body, our piece on recognizing diabetic peripheral neuropathy covers signs in the hands, autonomic system, and other regions. For more on the specific causes of foot numbness, see diabetes foot numbness causes.
From my experience: I have lived with type 1 diabetes for 14 years, and the first time I noticed something off in my feet was during a hike in my early thirties. My right sock was soaked with blood by the time we stopped for water, and I had no idea I had popped a small blister three miles back. That walk became the moment I built my evening foot check into a habit, the same way I check my CGM before bed. The exam takes about ninety seconds, costs nothing, and has caught two small issues before they became bigger ones.
Self-Examination: How to Check Your Feet
A daily foot check is the single most effective home tool for catching neuropathy changes early. The American Diabetes Association Standards of Care recommend daily inspection by patients and a thorough foot exam by a clinician at least once a year for people with diabetes.
Here is a routine that takes under two minutes once you have it down:
- Sit somewhere with good lighting, ideally after a shower or bath when the feet are clean and skin changes are easier to see
- Look at the tops of both feet, comparing color, hair pattern, and any new spots or swelling
- Lift each foot and check the soles, using a hand mirror or a phone camera if you cannot bend comfortably
- Spread each set of toes and look between them for cracks, peeling, or moisture
- Run a finger lightly across each part of the foot to feel for warm spots, cool spots, or numb patches
- Check your nails for thickness, color changes, or signs of fungal infection
- Note anything different from yesterday in a notebook or app
A monofilament test, where a thin nylon strand is pressed against the skin until it bends, is the standard clinical screen for protective sensation loss. Your podiatrist or diabetes educator can show you the technique, and home monofilament kits are inexpensive. Touching with a cotton ball, a slightly cool spoon, and a slightly warm spoon also gives a rough sense of whether sensation has changed across the seasons.
For more on building a sustainable daily foot care practice, our diabetic foot care guide walks through everything from drying technique to nail trimming.
What to Do If You Spot Something Concerning
The most important rule is this: do not perform home surgery. Do not pop blisters, do not scrape calluses, do not cut into ingrown toenails. The risk of infection in a foot with neuropathy is high, and a simple home intervention can become a hospital admission.
Document the change with a photo. A dated phone photo gives your podiatrist a baseline and lets them see how quickly something is progressing between visits. Take the photo from a consistent angle, with steady lighting, and keep it in a dedicated album.
Call your podiatrist or primary care provider promptly for any of these:
- A new ulcer or open wound, no matter how small
- A blister that did not have an obvious cause
- New redness, warmth, or swelling that does not fade overnight
- A callus with a dark center or any sign of bleeding underneath
- A change in foot shape or arch
- Pain, burning, or numbness that has worsened over a few weeks
- Any signs of infection, including fever, drainage, or a foul smell
Keep weight off the affected area until you are evaluated. If the issue is on the bottom of the foot, this may mean using crutches, a knee scooter, or simply staying off the foot as much as possible. Pressure on a small wound is what turns it into a large one.
Most serious foot complications in diabetes are preventable when changes are caught and addressed early. The combination of daily inspection, a low threshold for calling your care team, and steady blood sugar management makes the biggest difference over the years.
Building the habit that protects your feet
Pick a regular time for your foot check and tie it to something you already do, like brushing your teeth at night or sitting down to check your CGM. Keep a small mirror in the bathroom if bending is hard. Take a photo of any spot you are unsure about, and forward it to your care team if anything changes between visits.
Talk to your doctor about a baseline neurology exam if you have not had one in the last year, and ask about therapeutic footwear if calluses keep returning to the same spots. The pictures of diabetic neuropathy in feet that fill medical textbooks usually show late-stage disease. The version that matters for you is the one in your own bathroom mirror tonight, and the small adjustments that keep it from progressing.
FAQ
What does diabetic neuropathy look like in feet?
Early diabetic neuropathy in feet often shows up as subtle skin discoloration, hair loss on the toes, dry or shiny skin, calluses in unusual spots, and toenail changes. As it progresses, you may see toe deformities such as hammer toes, foot shape changes, blisters or ulcers, and in advanced cases, the rocker-bottom appearance of Charcot foot. Reference photos from medical sources can help you compare and identify what you see.
How do you tell if you have neuropathy in your feet?
Look for a combination of visible changes (skin color shifts, calluses, dry skin, nail changes) and sensory changes (numbness, tingling, burning, sensitivity to touch, balance trouble). A clinician can confirm with a monofilament test, tuning fork exam, and nerve conduction study. If symptoms appear in both feet symmetrically and start at the toes, diabetic peripheral neuropathy is the most likely cause.
When should you see a doctor about foot neuropathy signs?
Call your provider promptly for any new ulcer, blister, or open wound, for redness or warmth that does not fade overnight, for a callus with a dark center, or for sudden swelling or shape change in the foot. Worsening numbness, burning, or balance trouble over a few weeks is also worth a visit, even without a visible wound. Same-day evaluation is appropriate for signs of infection or for a Charcot foot pattern.
Can diabetic neuropathy in feet be reversed?
Established nerve damage usually cannot be reversed, but progression can be slowed or stopped with steady blood sugar management, healthy blood pressure and lipid levels, and active foot care. Some people see partial improvement in burning or tingling sensations after months of stable glucose readings. Talk to your doctor about your specific situation, as treatment options for symptom relief have expanded in recent years.
What is the difference between neuropathy and poor circulation in the feet?
Neuropathy is nerve damage and shows up as numbness, tingling, burning, or balance changes. Poor circulation is blood flow trouble and shows up as cold feet, pale or bluish skin, slow-healing wounds, leg cramping with walking, and weak pulses at the ankle. Many people with diabetes have both, since the same metabolic conditions damage nerves and blood vessels at the same time. A vascular and neurology exam together gives the clearest picture.
If you take one habit from this guide, make it the nightly check. The pictures of diabetic neuropathy in feet that show up in textbooks are usually advanced, but the version that matters most is the small change you spot tonight in your own bathroom mirror. Caught early, most of those changes have a clear path to action and a kind professional waiting on the other end of a phone call.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Health & Complications
View all
Diabetes and Dental Implants: What to Know First
Diabetes dental implants guide covering safety, A1C targets, recovery expectations, gum health prep, and what to ask your oral surgeon before surgery.

Burning Mouth Syndrome and Diabetes Explained
Burning mouth syndrome diabetes link explained, including neuropathy, dry mouth, and thrush causes plus treatment options that may bring real relief.

Dental Care for people with diabetes: Tips That Help
Practical dental care diabetics need, with real tips for protecting teeth and gums when diabetes raises your risk for oral health problems.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.