Sex and Diabetes: What to Know and What Actually Helps
Sex and diabetes is rarely covered honestly. Here is what changes for men and women, how to manage blood sugar around intimacy, and what actually helps.

In this article(8)
Sex and diabetes is one of those topics that gets brushed past in fifteen minute appointments and softened into clinical detachment in most articles. The reality is that diabetes can change how your body responds to arousal, how confident you feel during sex, and how your blood sugar behaves before, during, and after. Pretending otherwise leaves people quietly assuming something is wrong with them when, more often, something predictable is happening that has a name and a path forward.
We talk to people who have stopped initiating sex because they are afraid of going low, and to partners who have stopped asking because they do not want to feel like they are pushing. Both responses come from care, and both leave the relationship a little smaller. The point of this guide is to give you enough information to make different choices, with practical steps for the body and the conversation.
How Sex and Diabetes Affect Each Other
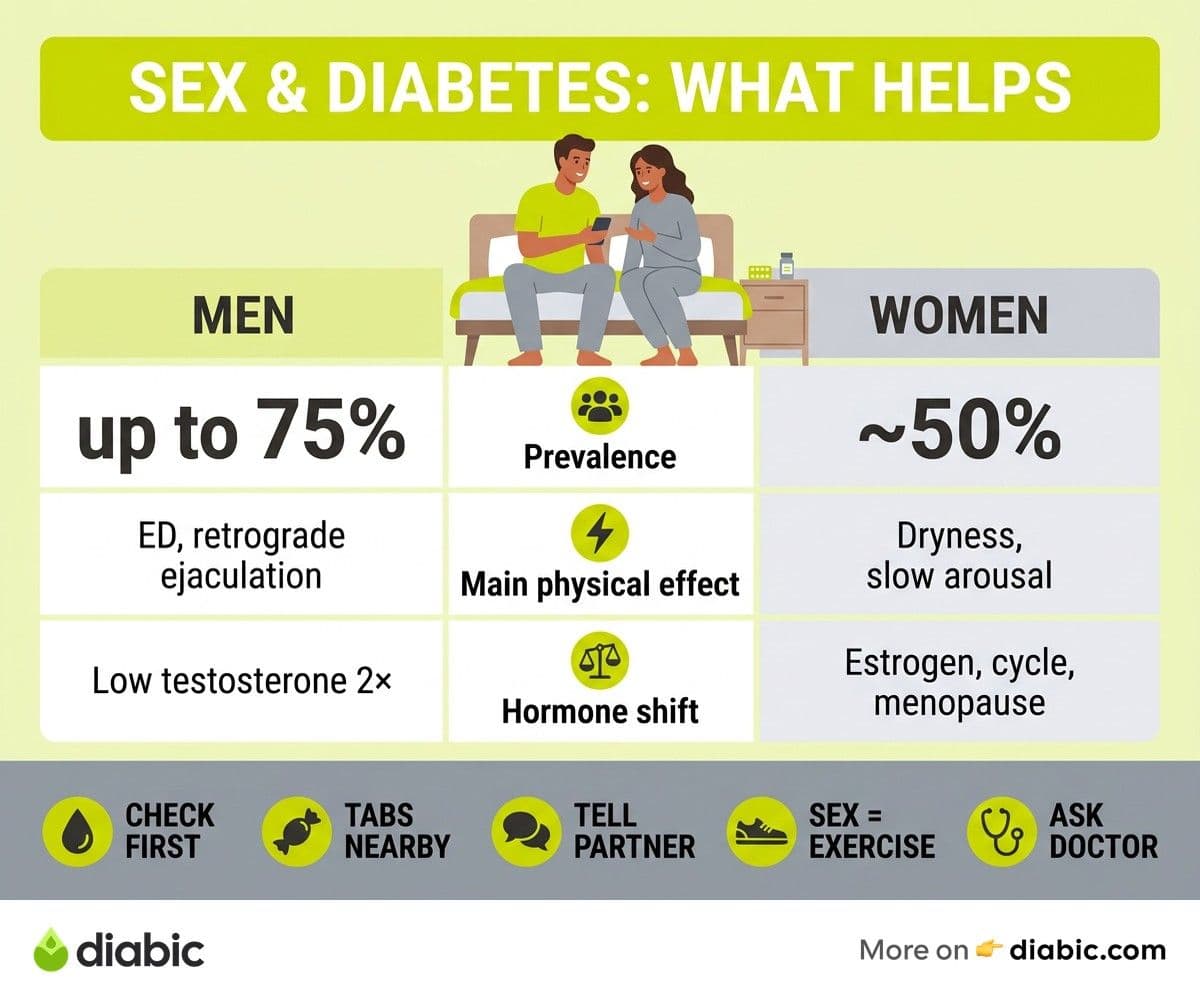
Sex and diabetes intersect in four main places, and most sexual concerns trace back to one or more of them. Nerve damage, called neuropathy, can dull sensation and slow arousal in both men and women. Blood vessel damage reduces the flow that erections, clitoral engorgement, and lubrication all depend on. Hormonal changes shift testosterone and estrogen in ways that quiet desire, and ordinary blood sugar swings drain the energy that intimacy needs.
The numbers behind this are larger than most people realize. The American Diabetes Association acknowledges that sexual dysfunction is one of the most common complications of diabetes, and research in Diabetes Care places lifetime prevalence of erectile dysfunction in men with diabetes at up to seventy five percent and the rate of female sexual dysfunction at roughly half. These rates do not mean a sentence. They mean that what you are noticing is shared by millions of people, and that clinicians know how to address most of it when asked.
The reason it goes underreported is simple. Most providers do not ask, most patients do not bring it up, and the appointment ends with a refilled prescription and an unspoken topic. We think the better default is to assume sexual health is part of diabetes care, and to talk about it the same way you would talk about feet, eyes, or kidneys. The body does not draw lines between which complications are polite to discuss.
Physical Effects in Men
Erectile dysfunction is the headline issue and the one that brings most men in. It tends to develop earlier and progress faster in diabetes than in the general population, and it is often the first sign that vascular and nerve health are changing. The mechanisms are mostly fixable when caught early, and our deeper guide on erectile dysfunction and diabetes covers PDE5 inhibitors, vacuum devices, injections, and lifestyle steps in detail.
Retrograde ejaculation is less talked about and more common than people assume. When autonomic neuropathy affects the bladder neck, semen can travel backward into the bladder rather than out, which is harmless but disorienting and a frequent cause of fertility concerns. The Urology Care Foundation has clear, non clinical write ups for both partners, and a urologist can usually distinguish this from other ejaculation issues in a single visit.
Low testosterone deserves its own line. It is roughly twice as common in men with type 2 diabetes as in the general population, contributes to fatigue, low libido, and reduced muscle mass, and is easy to test for. If your interest in sex has dropped along with your energy, asking for a morning testosterone level is a reasonable starting point. Treatment, when appropriate, is straightforward and managed by an endocrinologist or urologist, not something you need to navigate alone.
Physical Effects in Women
The picture for women is less studied and equally real. Vaginal dryness, slower arousal, and difficulty reaching orgasm all show up at higher rates with diabetes, partly from reduced pelvic blood flow and partly from hormonal shifts. The International Society for the Study of Women's Sexual Health has patient resources covering everything from over the counter lubricants to prescription topical estrogen, and most of these solutions are inexpensive and quietly effective.
Recurrent yeast infections and urinary tract infections compound the problem, because elevated glucose creates an environment where these infections thrive, and discomfort changes how the body anticipates sex. If you find yourself bracing rather than relaxing, that is a physiological pattern your nervous system has learned, not a personal failing. Treating the infections aggressively and stabilizing glucose tends to interrupt the cycle within a few months.
Desire and arousal are influenced by hormones in ways that often go unexamined in diabetes care. Cycle changes, perimenopause, and menopause all interact with insulin resistance, and our guide on libido and blood sugar walks through how those threads tie together. The takeaway for now is that vaginal symptoms, low desire, and difficulty with orgasm are medical issues with concrete options, not something to endure quietly.
Managing Blood Sugar Around Intimacy
This is the section we wish someone had written for us a long time ago. Sex is physical activity, and like any physical activity, it lowers blood sugar. The tricky part is that arousal can also raise glucose briefly through adrenaline, and the timing varies between people, so the only way to learn your pattern is to watch a few sessions and treat the data the same way you would treat exercise data.
For continuous glucose monitor users, placement matters. Sensors on the upper arm are usually fine, while sensors on the abdomen can be uncomfortable depending on positions. Adhesive patches over the sensor reduce the chance of it pulling loose, and most people find that the sensor reads accurately during and after sex. If you use an insulin pump, decide in advance whether you will disconnect, switch to a lower temporary basal, or leave things as they are. There is no single right answer. Some pump users disconnect for up to an hour without issue, others find that even a small basal reduction prevents post sex lows.
A few practical habits remove most of the surprise. Check your blood sugar before sex, and aim for a starting point a little higher than your usual target if it has been a few hours since you ate. Keep fast acting glucose, juice or glucose tabs, on the nightstand within reach so neither of you has to leave the room if a low arrives.
From my experience: A few years into using a Dexcom G6, I learned the hard way that a delayed low can show up an hour after sex on a night I had also walked the dog. Now my routine is simple: a glance at the CGM curve, glucose tabs already on the nightstand, and a small snack with peanut butter afterward if my arrow is pointing down. Saying it out loud to my partner once, instead of leaving them to guess what the buzzing sensor meant, took more pressure off both of us than any device tweak ever did. Eat a small snack with protein afterward if sex was longer or more energetic than usual, since delayed lows can show up an hour or two later, especially overnight. Our guide on how diabetes affects intimacy covers more of these everyday adjustments.
Communication is the part that ties it all together, and it is also the part most couples avoid. Telling a partner what a low feels like, what helps, and what you would like them to do or not do during one removes a huge amount of background anxiety for both of you. The same is true for visible devices, scars, and any changes in sensation or response. Most partners want to know. They are usually waiting to be told it is okay to ask.
When to Talk to Your Doctor About Sexual Health
Your provider can help, but in most clinics they will not raise the topic on their own, so the responsibility to start the conversation lands on you. The good news is that you do not need a long speech. A direct sentence works. Something like, my sex drive has dropped over the past six months and I want to figure out why, gives the visit a clear direction and signals that this is a real concern, not a passing comment.
Be specific about what has changed and when it started. Bring the timeline, any patterns you have noticed with blood sugar, and a list of medications, since several common diabetes adjacent prescriptions, including some blood pressure drugs and SSRIs, can affect sexual function. Ask about referrals where appropriate. A urologist for men, a gynecologist or pelvic floor physical therapist for women, an endocrinologist for hormone questions, and a therapist who specializes in sexual health or chronic illness are all reasonable next stops.
Treatment options have widened in recent years and include PDE5 inhibitors for erectile dysfunction, hormone therapy where indicated, topical estrogen and lubricants for vaginal symptoms, pelvic floor therapy for both men and women, and various devices that support arousal and orgasm. The American Association of Sexuality Educators, Counselors and Therapists maintains a directory of vetted therapists if the emotional or relational piece is what most needs attention. Our guide on hormonal changes from diabetes is a good companion read before that appointment.
Frequently Asked Questions
How does diabetes affect your sex life?
Diabetes can affect sex through nerve and blood vessel changes, hormone shifts, blood sugar swings, and the emotional load of managing a chronic condition. In men, this most often shows up as erectile dysfunction, low libido, or ejaculation changes. In women, it tends to appear as vaginal dryness, slower arousal, recurrent infections, and difficulty with orgasm. The effects are common but rarely permanent without treatment, and most people can recover meaningful function with a combination of glucose stability, medical evaluation, and honest conversation with a partner.
Can diabetes cause sexual problems?
Yes, and the link is well established. Up to seventy five percent of men with diabetes will experience erectile dysfunction at some point, and roughly half of women with diabetes report at least one form of sexual dysfunction. The good news is that almost all of these issues have effective options when raised with a provider, and many improve with the same steps that improve overall metabolic health, including stable blood sugar, regular movement, sleep, and addressing depression and anxiety. The earlier you bring it up, the more options you usually have.
The point of all of this is not to add another item to a long list of things to manage. It is to take a topic that has been kept quiet, often at real cost to relationships and self image, and put it back in the same room as the rest of your care. Sex and diabetes can coexist well. The first step is usually just naming what has changed, out loud, to someone who can help.
Shahriar P. Shuvo is the founder of Diabic. He has lived with diabetes for over 14 years, and built Diabic to deliver the practical, evidence-based self-management tools he wished existed when he was first diagnosed. By trade, Shahriar is a senior design and frontend engineer with 6+ years shipping products at Agora, Timescale (now Tiger Data), and ShareTrip. He writes from the intersection of lived diabetes experience and product craft, focused on what works in daily management rather than what sounds good in a textbook.
Medically reviewed by
Dr. Shanto Arian is an internal medicine physician now specializing in clinical and aesthetic dermatology, with a parallel academic focus on epidemiology and public health. He holds an MBBS, MPH, MSc (UK), MRCP (UK), MRCPI (Ireland), Diploma in Dermatology (UK), and Diploma in Aesthetic Medicine (USA). Dr. Arian trained in internal medicine, including hospital work on hematology cases such as graft-versus-host disease, before moving toward dermatology. Skin is one of the earliest places diabetes shows itself, from acanthosis nigricans and diabetic dermopathy to slow foot wound healing, and that intersection is where his clinical and Diabic-review work meet. On Diabic, Dr. Arian medically reviews content on diabetes diagnosis, complications, dermatologic manifestations, and pharmacotherapy, ensuring every claim aligns with current ADA, NICE, and peer-reviewed literature.
More from Living with Diabetes
View all
Generic vs Brand Insulin: Is There a Difference?
Generic vs brand insulin compared: how biosimilars are approved, what you save with Semglee or ReliOn, and how to talk to your doctor about switching.

Patient Assistance Programs for Diabetes Medication
Patient assistance programs diabetes patients qualify for can cut prescription costs to little or nothing. Here is how to find and apply for them.

Diabetes Supply Savings Tips That Actually Work in Real Life
Practical diabetes supply savings tips for cutting costs on test strips, CGMs, insulin, and pump supplies without compromising your care.
Clinician-reviewed habits, plain-language guides, and honest answers - the small shifts that make living with diabetes feel lighter, every day.